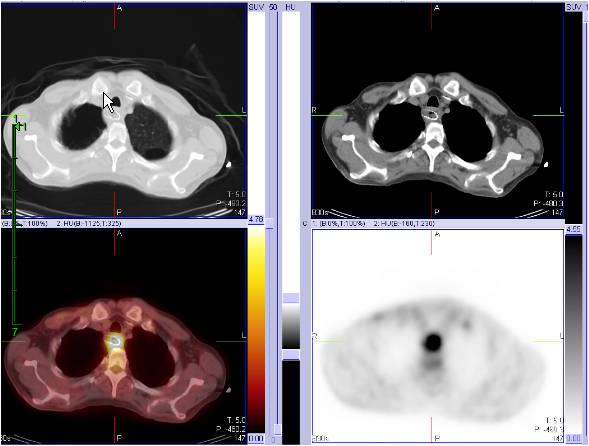
| Findings: Initial PET-CT:
RADIOPHARMACEUTICAL: 15 mCi F-18 Fluorodeoxyglucose i.v.
Two foci of markedly increased FDG uptake in the thickening of the mid esophagus, suspicious for malignancy.
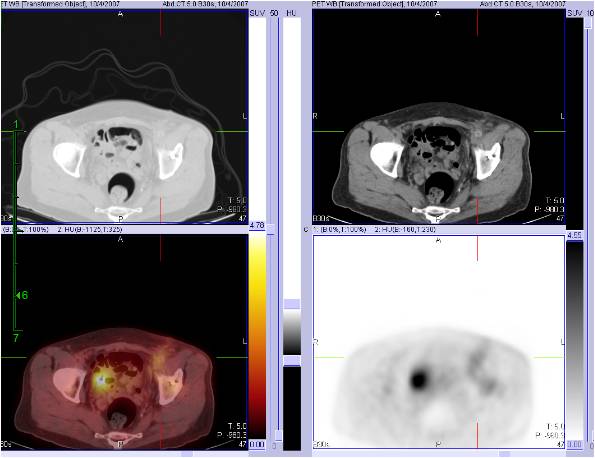
Follow up PET-CT:
RADIOPHARMACEUTICAL: 13.6 mCi F-18 Fluorodeoxyglucose i.v.
1. Two persistent foci of markedly increased FDG uptake involving theĀthickenedĀmid esophagus, not significantly changed.
2. Multiple new rib and sternal fractures, likely related to cardiac resuscitation.
3. Diffuse mild increased FDG uptake in the left inguinal soft tissue, likely inflammatory in nature and related to vascular catheterization.
4.ĀFree intraperitoneal air related to recent laproscopic procedure.
|