|
| Patient: 60 year old female |
| History: 61-year-old female with small cell lung cancer and prior intracranial metastatic disease. |
Image Size:
|
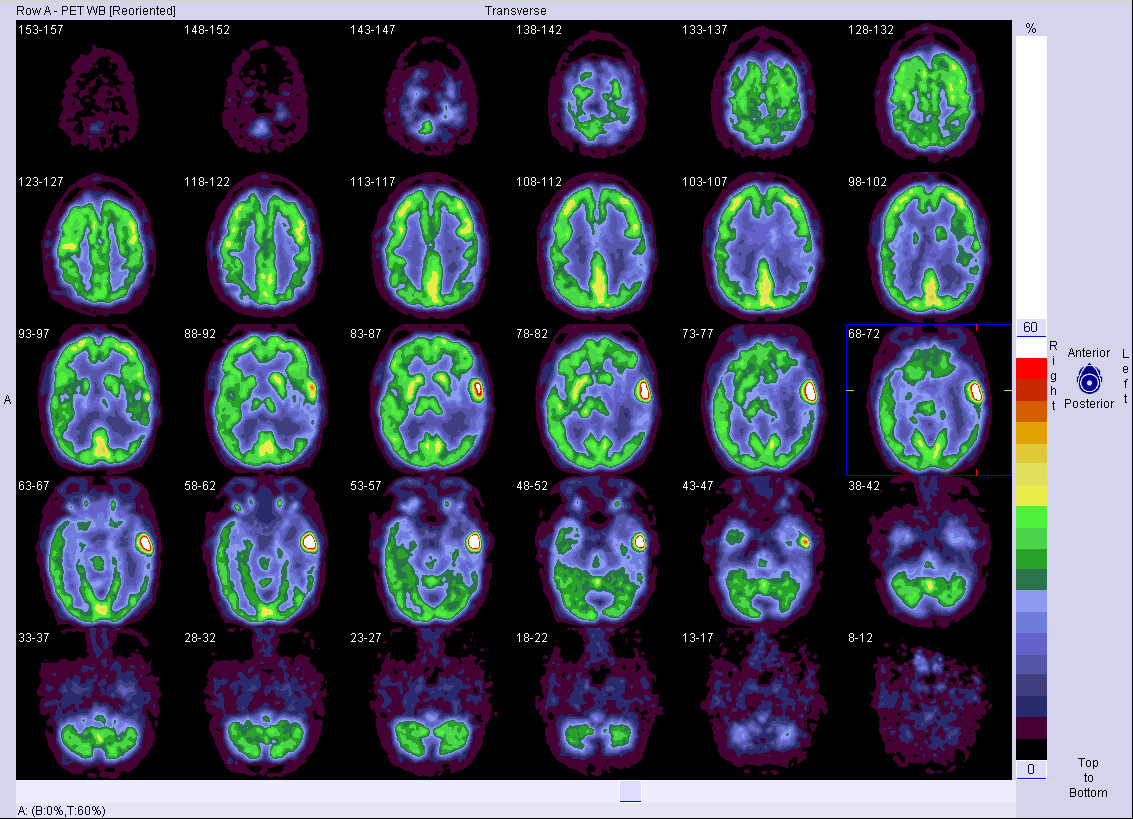
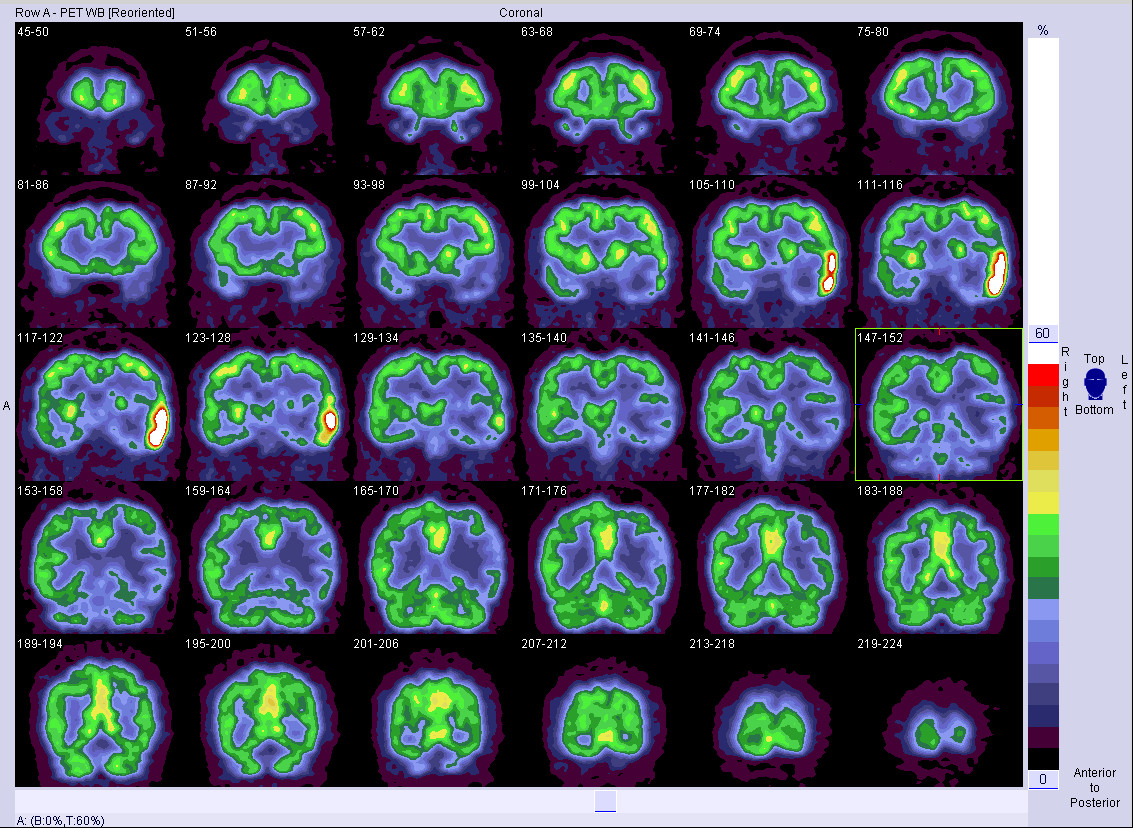
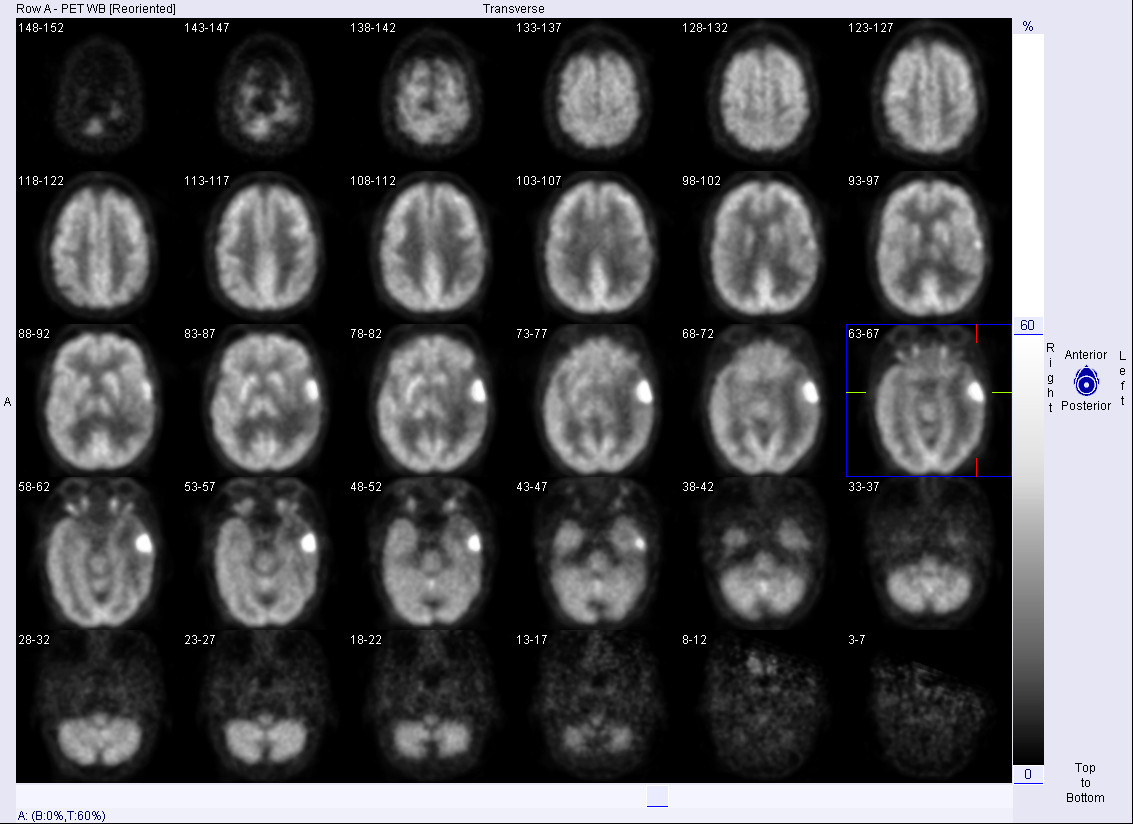
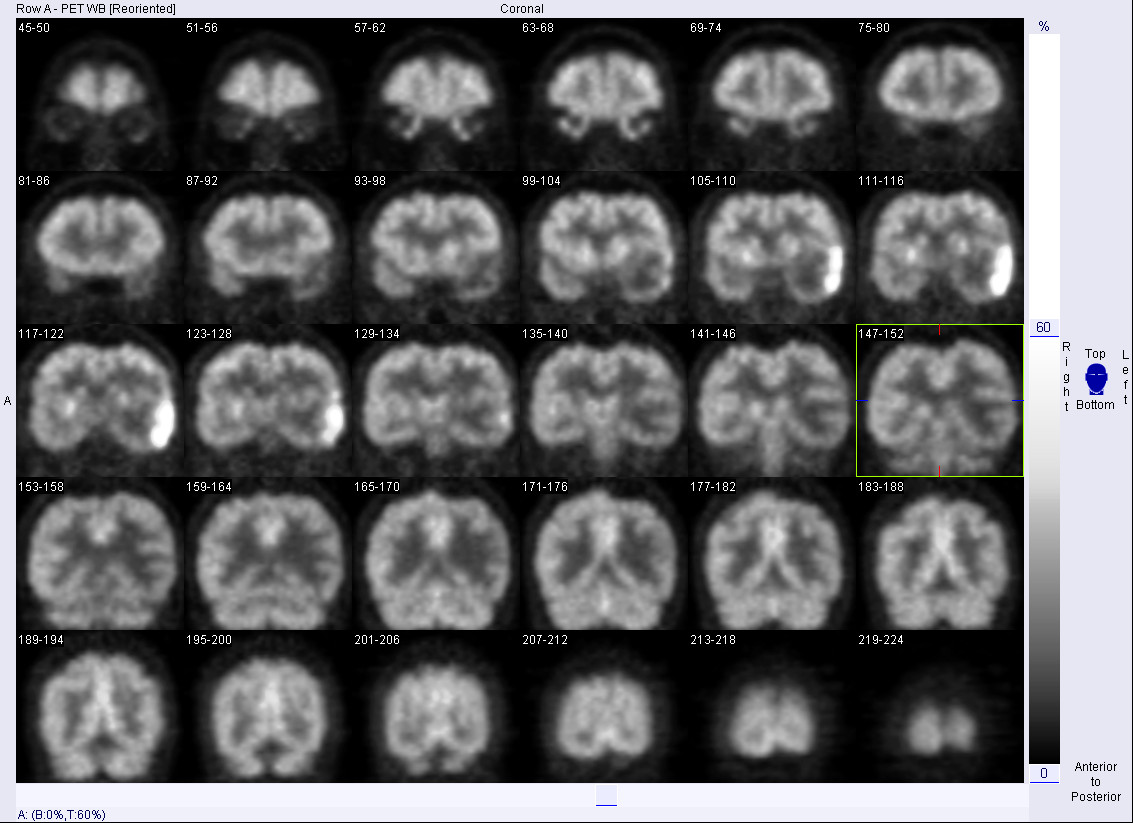
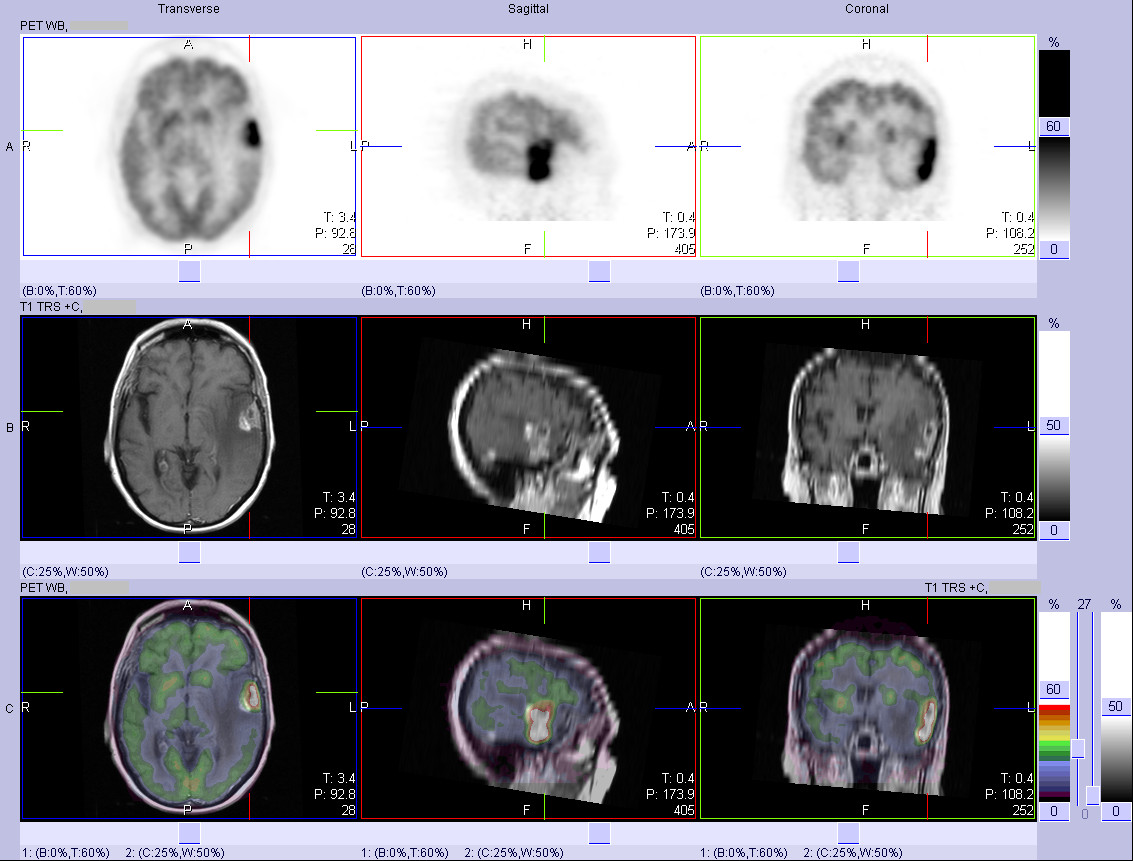
| Findings: FDG PET: Highly FDG avid left temporal mass, with mild surround hypometabolism. No other lesions.
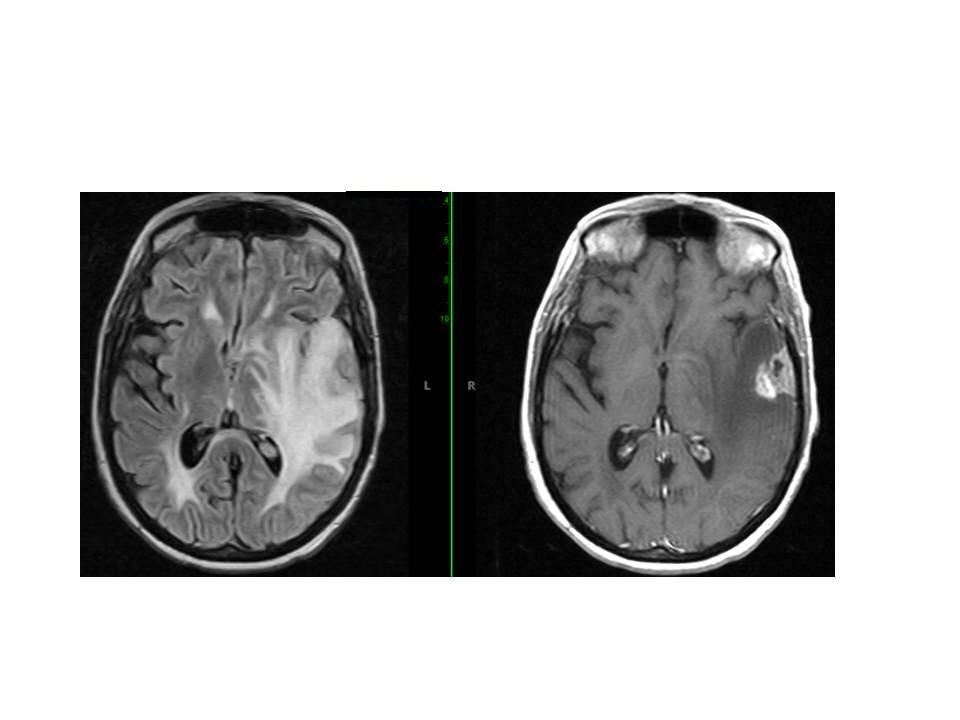
Brain MRI: Left temporal lobe mass with maximal axial dimension of 4.1cm, with surrounding vasogenic edema. Mild midline shift to the right of 5 mm. |
| DDx: Recurrent or residual brain metastatic disease
Primary brain tumor
Infection/Herpes encephalitis
Lymphoma |
| Diagnosis: Recurrent or residual brain metastatic small cell carcinoma |
| Comments: No comments posted. |
| Additional Details:
Case Number: 114581 The reader is fully responsible for confirming the accuracy of this content. |