General Discussion: Long history: 56-year-old woman who presents with weight loss and bloody diarrhea. She had recurrent intermittent lower gastrointestinal bleeding. The patient is transferred from an outside hospital for decreased HCT. The HCT was 17% during the first few days of the admission and she required numerous tranfusions and two separate ICU stays during admission. Evaluate for bleeding source.
Radiopharmaceutical: 27.01 mCi Tc-99m in vitro labeled red cells i.v.
Angiography: No active extravasation or definite abnormal vascularity was identified on the mesenteric angiogram.
Follow up: Small bowel enteroscopy shows an oozing linear jejunal ulcer with a visible vessel in the proximal jejunum.
Surgical Pathology Report: The jejunal biopsy revealed moderate villous blunting
and increased chronic inflammatory cells in the epithelium and lamina propria.
Granulomas are absent. These findings are not specific, but are consistent with
Crohn's enteritis.
Discussion: Bleeding from the small bowel is a rare cause of GI blood loss. Cancers, inflammatory bowel disease, and infection account for 20-25% of all small bowel bleeding, while AVMs account for the vast majority of bleeds.
Determining the source of gastrointestinal bleeding that originates in the small bowel is one of the major diagnostic challenges facing gastroenterologists because the small bowel is long and hard to reach by endoscopy and therefore difficult to evaluate.
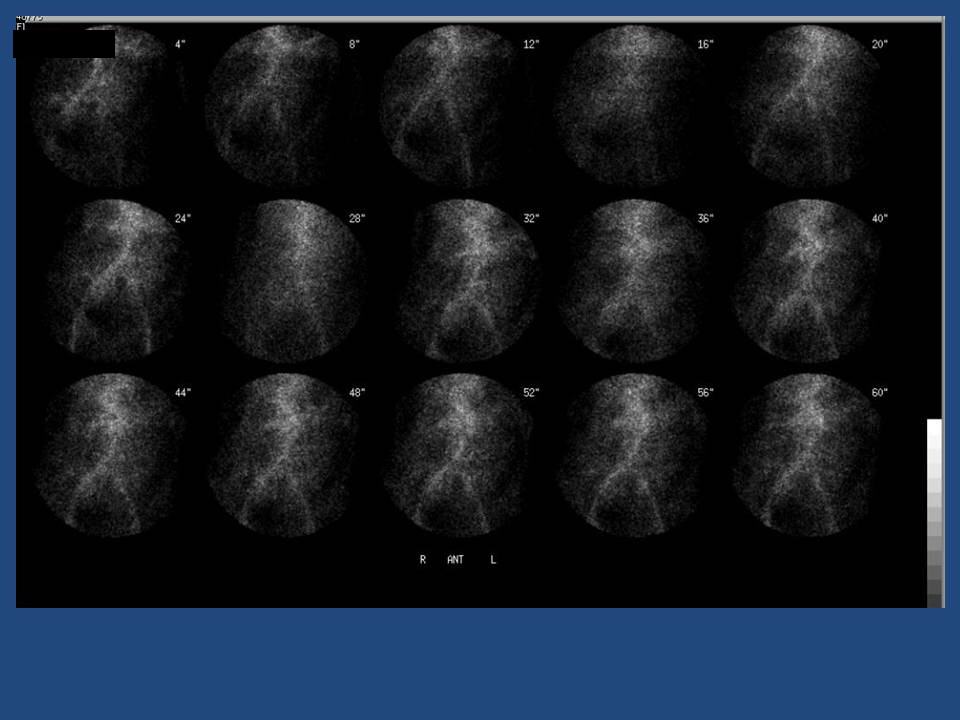
The GI bleeding scintigrahic study is to diagnose and localize the site of bleeding. Over 80% of bleeding sites are detected during the initial imaging. The activity persists and travels anterograde into loops of small bowel during the reemaider of the imaging period. This is most likely in the proximal portion of the jejunum.