Case Author(s): Zhiyun Yang, M.D., and Tom R. Miller, M.D., Ph.D. , 04/16/05 . Rating: #D3, #Q3
Diagnosis: PET in Systemic Lupus Erythematosis
Brief history:
57-year-old woman with a diagnosis of B-cell non-Hodgkin's lymphoma presents for restaging.
Images:
Coronal FDG-PET images
View main image(pt) in a separate image viewer
View second image(pt).
Axial FDG-PET images
View third image(pt).
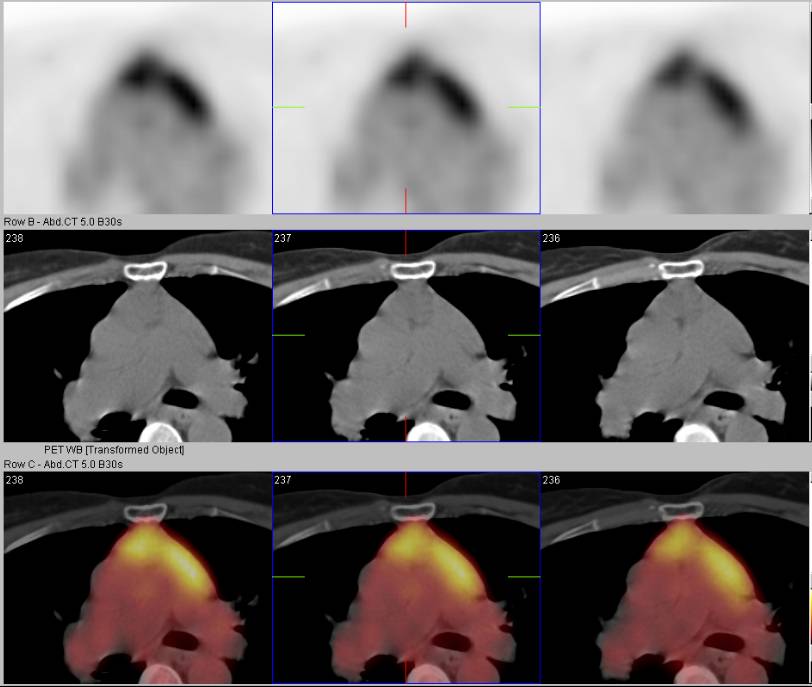
Fused PET-CT images
View fourth image(pt).
Comparion of two fused PET-CT images
Full history/Diagnosis is available below
Diagnosis: PET in Systemic Lupus Erythematosis
Full history:
This 57-year-old woman was diagnosed with B-cell non-Hodgkin's lymphoma. The patient completed treatment in 2000. In 2003 the patient was found to have an anterior mediastinal mass, which was biopsied in 2004 at an outside hospital, showing no recurrent lymphoma. The patient has a history of Lupus. Restaging of lymphoma is requested by PET/CT.
Radiopharmaceutical:
14.9 mCi F-18 Fluorodeoxyglucose i.v.
Findings:
There is an area of intense uptake within the anterior mediastinum at the level of the pulmonary artery, corresponding to an anterior mediastinal mass on CT. The appearance is unchanged compared with the previous study obtained in 8/04.
Mild uptake is also present within multiple subcentimeter lymph nodes in the posterior cervical triangle and about the parotid glands bilaterally. Their appearance also is unchanged compared with the previous study. Mild uptake is seen in right and left axillary subcentimeter lymph nodes, unchanged from the previous study.
Discussion:
In this case, the PET/CT shows a predominantly stable appearance of increased uptake within the anterior mediastinum, and bilateral neck, and bilateral axillary lymph nodes. Given the report of the patient's negative anterior mediastinal mass biopsy and the patient's history of Lupus, coupled with the fact that these masses have been stable since August, 2004 and, by report also unchanged on an outside PET study in 2003, these lesions may represent the sequela of Lupus rather than recurrent lymphoma.
The study of Nowak et al. demonstrated two important findings. First, compared with healthy controls, both patients with active Lupus and those with inactive Lupus had increased FDG uptake in lymph nodes. This suggests that metabolic, and probably immunologic, activity is enhanced not only in active, but also in clinically quiescent disease. Second, thymic uptake is increased in patients with active Lupus, but not in those with inactive disease. This intriguing observation suggests a quantitative difference in the immune response in different stages of clinical activity and provides evidence for an important role of the thymus during active disease.
Reference:
Nowak M, Carrasquillo JA, Yarboro CH,et al. A pilot study of the use of 2-(18F)-fluoro-2-deoxy-D-glucose-positron emission tomography to assess the distribution of activated lymphocytes in patients with systemic lupus erythematosus. Arthritis Rheum. 2004 Apr;50(4):1233-8.
Followup:
The referring physician suspected that the original diagnosis of lymphoma, made at another hospital, may have been in error. Thus, in view of the stable findings over several years without treatment, the PET/CT findings most likely are do to Systemic Lupus Erythematosis, as observed in the study of Nowak et al.
Differential Diagnosis List
Recurrent lymphoma, active Lupus.
ACR Codes and Keywords:
References and General Discussion of PET Tumor Imaging Studies (Anatomic field:Lung, Mediastinum, and Pleura, Category:Neoplasm, Neoplastic-like condition)
Search for similar cases.
Edit this case
Add comments about this case
Return to the Teaching File home page.
Case number: pt134
Copyright by Wash U MO
{kind=link}
{kind=link}
{kind=link}