|
| Patient: 41 year old female |
| History: 41-year-old woman with recurrent cervical cancer status post radical hysterectomy and pelvic lymph node dissection on 07/27/2010 and chemoradiation therapy presenting with feculent discharge per vagina. She is diagnosed to have bilateral hydronephrosis.
|
Image Size:
|
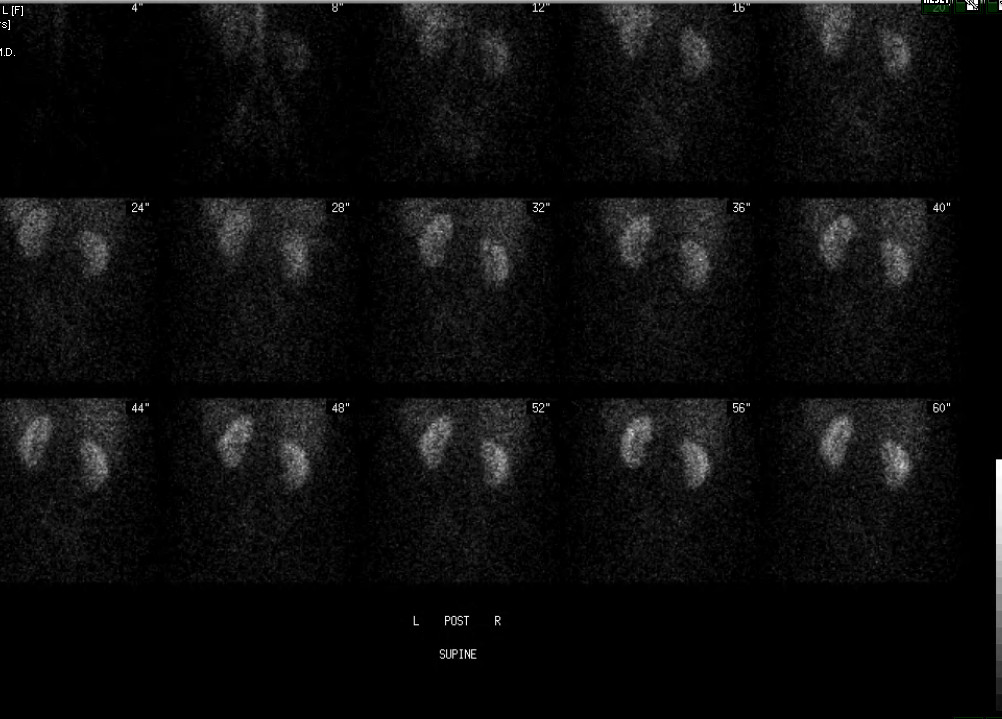
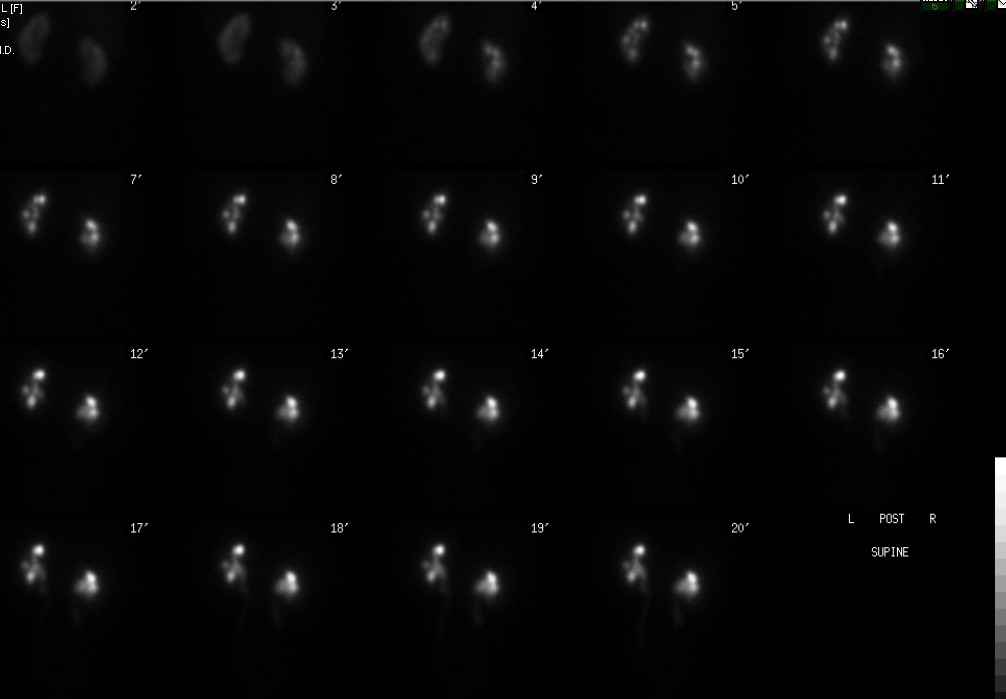
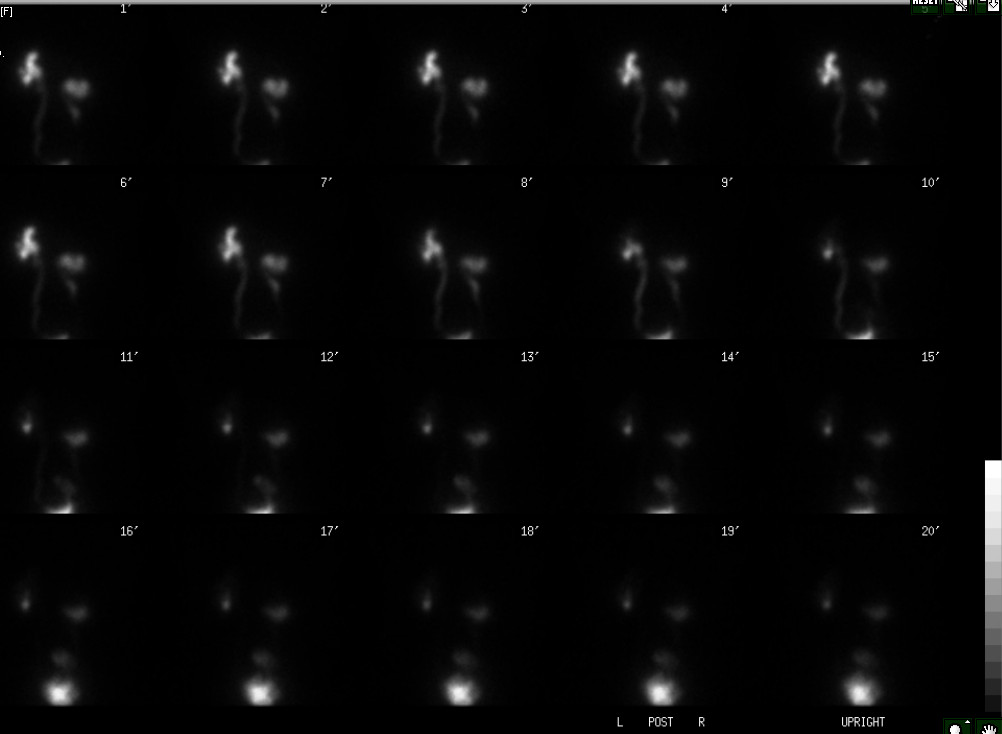
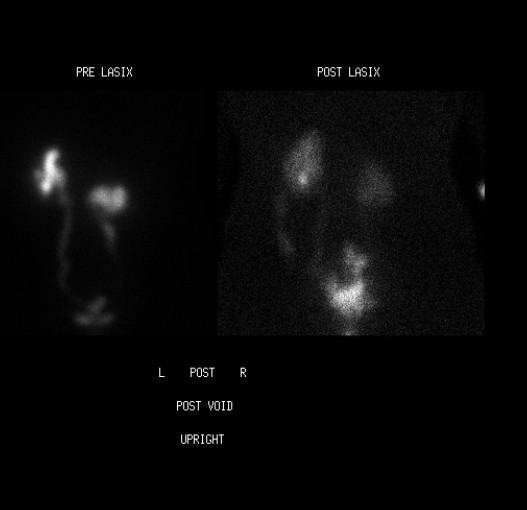
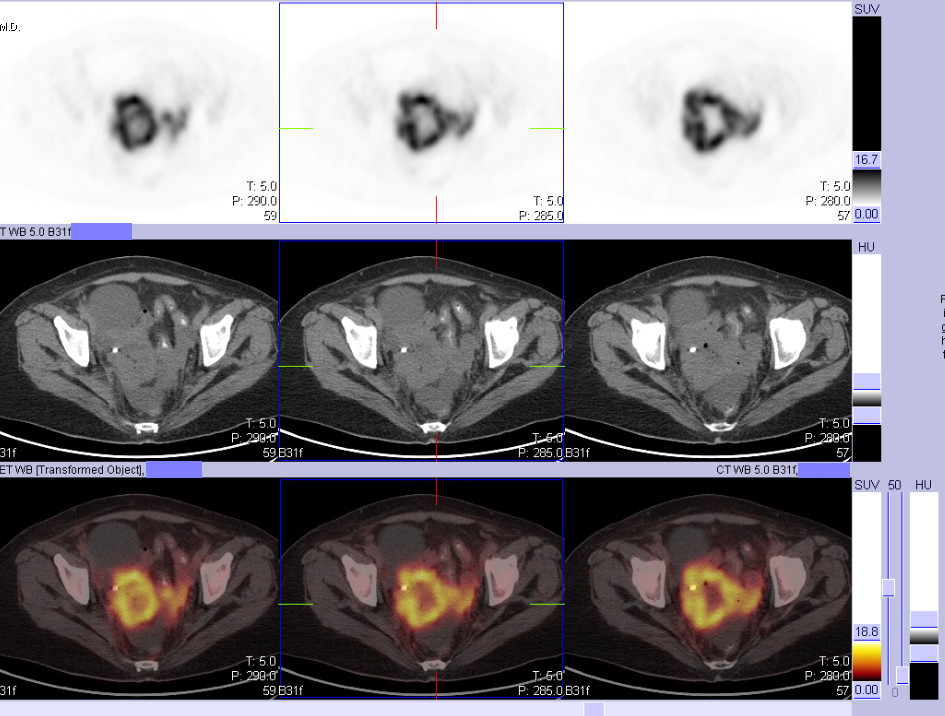
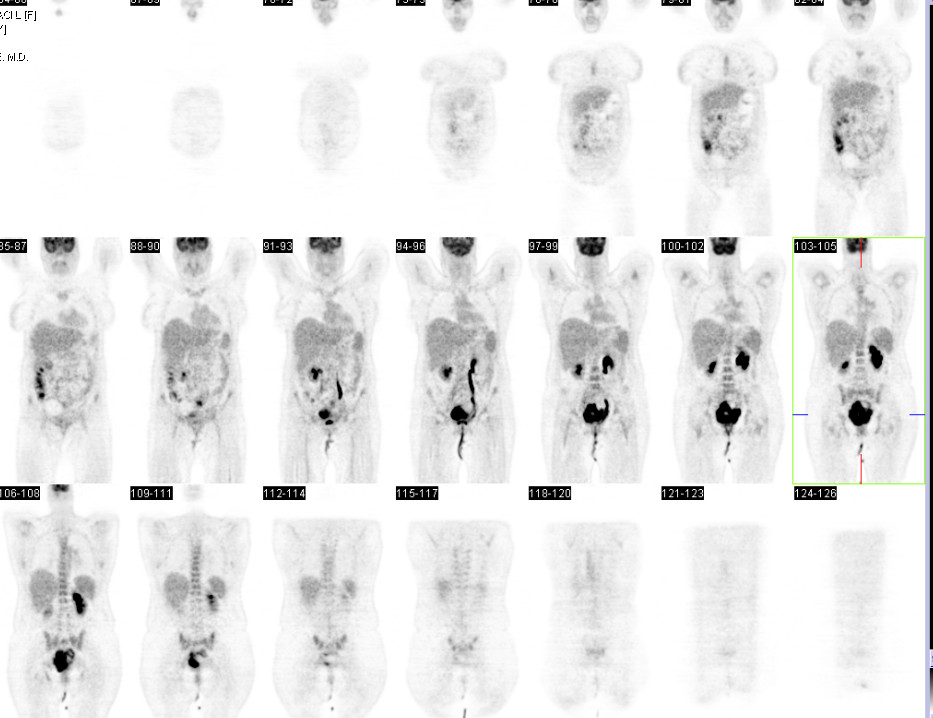
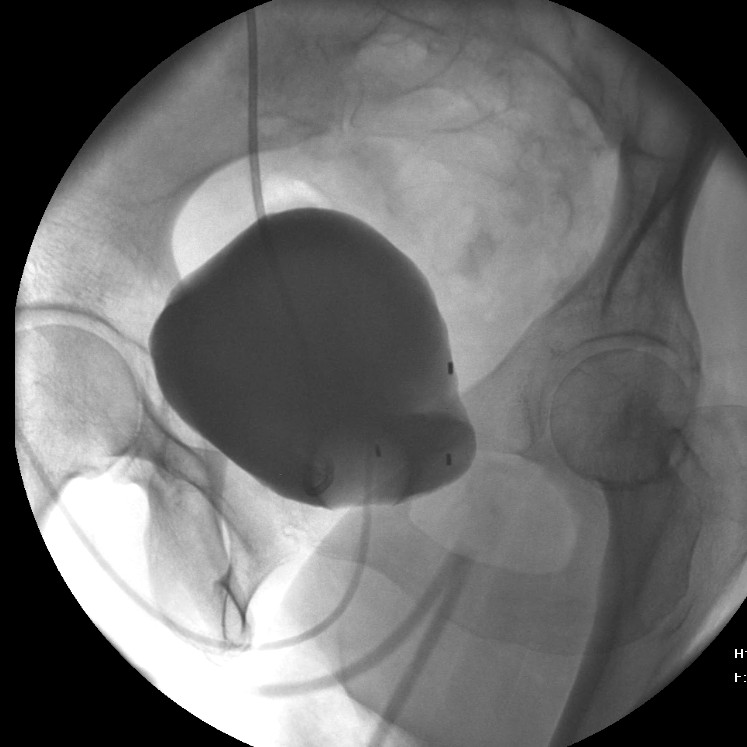
| Findings: Renal scan: After 20 minutes of imaging, there is a small amount of retained activity in the left collecting system, which appears mildly enlarged There is a small amount of retained activity in the right collecting system, which appears mildly enlarged. Static images were then obtained after erect positioning and voiding. There is mild retained activity in bilateral collecting system. There is moderate activity in the lower pole calyx of the left collecting system. The right kidney appears ptotic. The left ureter appears dilated. The right ureter appears dilated and is tortuous in the distal part. The bladder is distended and there is focal collection extending from superior and lateral to the urinary bladder on the right side, and to the right lower quadrant. The activity is seen arising from the superolateral aspect of the urinary bladder. The estimated contribution of the right kidney to total renal function is 48% and that of the left kidney is 52% To evaluate for obstruction, the patient was given furosemide via slow intravenous injection approximately 20 minutes after the start of the examination. Sequential images were obtained for an additional 20 minutes with the patient in the erect position. There is prompt clearance of pelvicalyceal activity on the left after diuretic administration. On the right, there is mildly delayed clearance of activity from the pelvicalyceal system. After diuretic administration, the half-time of tracer clearance from the right kidney is 13 minutes and from the left kidney is 2 minutes. IMPRESSION: 1. Normal renal perfusion, function, with mildly dilated collecting system on both sides. 2. No evidence of significant obstruction of either kidney. 3. Focal activity arising from the superolateral aspect of the bladder, with extension into the right lower quadrant, most likely represents urinoma. PET/CT: 1. Large hypermetabolic pelvic mass compatible with invasive recurrent cervical cancer. 2. Hypermetabolic mesenteric and right external iliac lymph nodes compatible with nodal metastatic disease. 3. Bilateral hydronephrosis, left greater than right. 4. Multiple cystic pelvic masses, likely representing lymphoceles. CYSTOGRAM: No evidence of contrast extravasation from the urinary bladder. COMPUTED TOMOGRAPHY OF THE ABDOMEN AND PELVIS WITH AND WITHOUT INTRAVENOUS CONTRAST (CT UROGRAPHY): Large fungating pelvic mass with central necrosis which engulfs the distal left ureter with extravasation of contrast from the ureter into the central necrotic portions of the mass and caudally into the vagina consistent with a ureterovaginal fistula. Collection of radiotracer within the necrotic mass likely explains the findings on recent nuclear renal scan. Water-soluble contrast enema: 1. Colovaginal fistula in the distal sigmoid colon and proximal vagina. 2. Marked contour irregularity and narrowing within the sigmoid colon, which very likely is related to the patient's known pelvic mass. |
| DDx: 1. Post operative seroma. 2. Urinoma. 3. Lymphocele. |
| Diagnosis: •Rectovaginal and ureterovaginal fistula. Pelvic Lymphoceles.
|
| References: 1. Priya Narayanan, MBBS, Marielle Nobbenhuis, MBBS, Karina M, Reynolds, FRCOG, Anju Sahdev, MD, Rodney H. Reznek, MBBCh, Andrea G. Rockall, MBBS, Fistulas in Malignant Gynecologic Disease: Etiology, Imaging, and Management, July 2009 RadioGraphics, 29, 1073-1083. 2. Nicola Mumoli,and Marco Cei, Clinical picture: Ureteral urinomaQ J Med 2010; 103:623–624. 3. Helen C. Addley, MRCP, FRCR • Hebert Alberto Vargas, MD • Penelope L. Moyle, MBChB • Robin Crawford, MD, FRCS, FRCO, Evis Sala, MD, PhD, FRCR, Pelvic Imaging Following Chemotherapy and Radiation Therapy for Gynecologic Malignancies, RadioGraphics 2010; 30:1843–1856. 4. Ross L. Titton, MD, Debra A. Gervais, MD, Peter F. Hahn, PhD, MD, Mukesh G. Harisinghani, MD, Ronald S. Arellano, MD, Peter R. Mueller, MD, Urine Leaks and Urinomas: Diagnosis and Imaging-guided Intervention, RadioGraphics 2003; 23:1133–1147 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 305816 The reader is fully responsible for confirming the accuracy of this content. |