|
| Patient: 54 year old female |
| History: 55 year oldĀfemale with recently diagnosed breast cancer on routine screening mammography. Chest, abdomen and pelvis CT scan was performed as part of initial staging. |
Image Size:
|
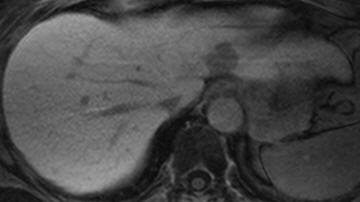
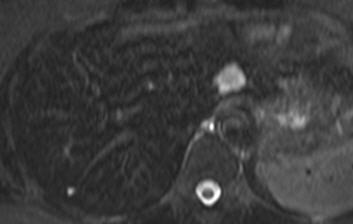
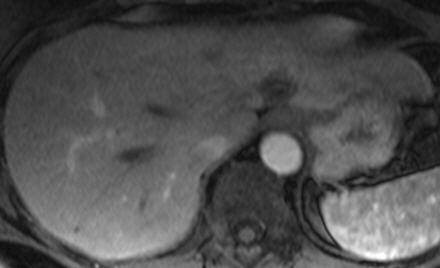
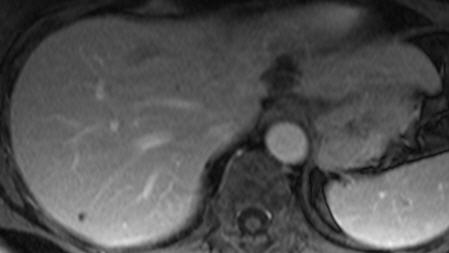
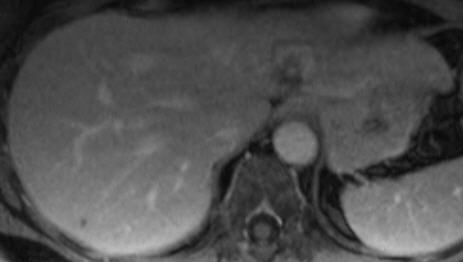
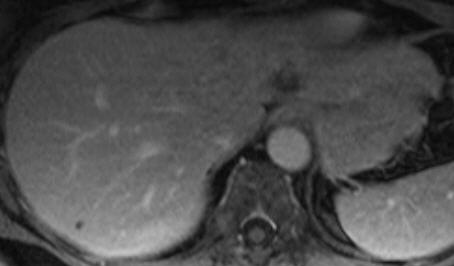
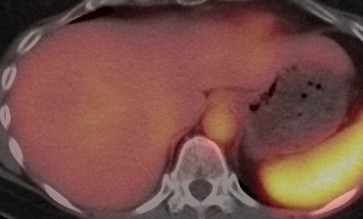
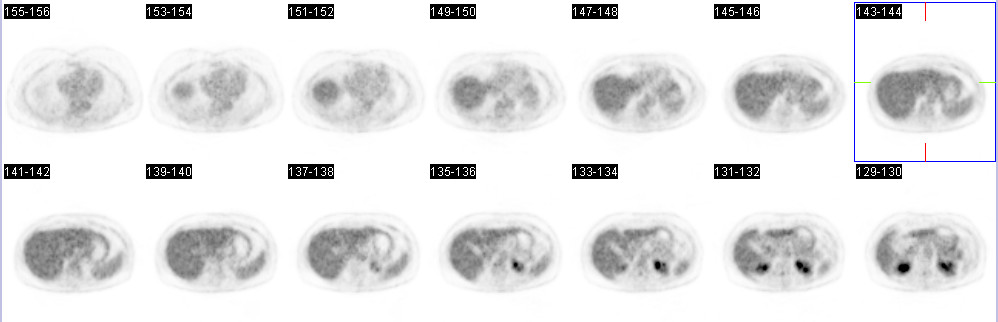
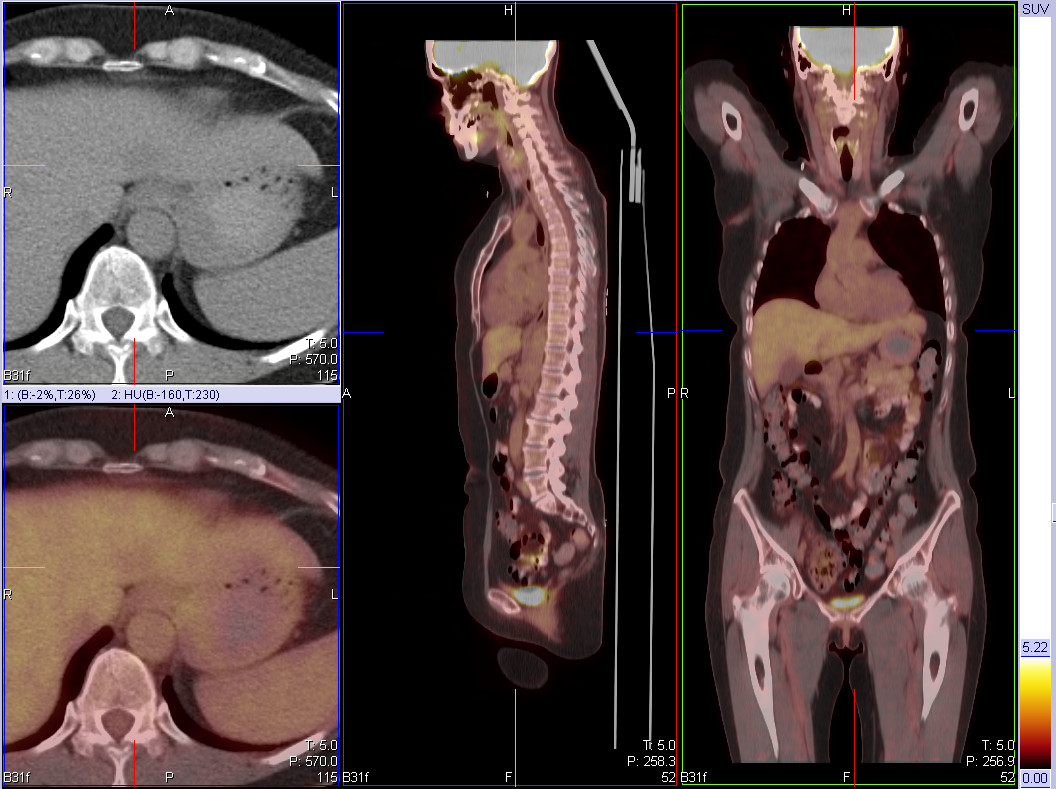
| Findings: Contrast enhanced CT image at the level of the upper abdomen is presented (Fig 1). Identify the phase in which the scan was preformed and the finding. The contrast enhanced axial CT image at the venous phase shows a hypodense lesion in segment 2 of the liver (Fig 1). Non-enhanced scan as well as multiphase, arterial and delayed images, were not acquired in this study, so the pattern of enhancement seen at the posterior aspect of the lesion can not be well characterized. What is the main differential diagnosis?In the context of this patient medical history the main differential diagnosis include benign lesion such as hemangioma vs metastatic lesion. Hepatic cyst is unlikely considering the impression of peripheral, somewhat nodular enhancement at the posterior aspect of the lesion. Primary liver neoplasm is also less likely. Presented are MRI images of the lesion at different sequences and contrast phases (Fig 2-7). Is the diffrential diagnosis narrowed?Ā Typical hemangioma is a well marginated lesion iso or hypointense to blood on T1 and hyperintense (similar to CSF) on T2. The typical pattern of enhancement is peripheral, nodular, discontinuous enhancement on arterial phase with progressive centripetal filling on the venous phase. On both arterial and venous phase it is isointense to blood. On delayed phases there is persistent complete filling. Atypical hemangioma, hyalinized (sclerosed) hemangioma and hemangioma in cirrhotic liver demonstrate different pattern of enhancement. Atypical hemangioma presents inside to outside enhancement pattern, centrifugal filling. Sclerosed or hyalinized hemangioma can show only minimal enhancement and therefore cannot be diagnosed with confident by imaging. Small hemangioma in cirrhotic liver may show homogenous enhancement and mimic HCC. Hemangioma in cirrhotic liver may become more fibrotic and lose the characteristic pattern of enhancement. In our case the lesion is well marginated and hypointense to blood on T1 weighted image (Fig 2)Āand hyperintense on T2 weighted image (Fig 3). On arterial phase there is peripheral enhancement within the anterior aspect of the lesion, but unlike typical hemangioma is not isointense to blood (Fig 4). There is also central enhancement seen on portovenous (Fig 5, Fig 6) and delayed phase (Fig 7) as well as gradually peripheral enhancement. Hypovascular metastatic lesions are usually hypointense on T1 and moderately to highly intense on T2. The typical pattern of enhancement is peripheral rim with low signal center indicating vascularized viable tumor in the periphery and hypovascular or necrotic center. The lesion presented in this case does not demonstrate the classic imaging findings of typical hemangioma, nevertheless there are some characteristic findings of atypical hemangioma. Most breast cancer are hypovascular, and the pattern of central and peripheral enhancement of this single lesion is not typical to hypovascular metastasis. What are the other imaging modalities available to evaluate this lesion? Tc-99m labeled RBC with SPECT is considered accurate modality for diagnosing hemangioma. Presented are three one hour delayed images of 20.8 mCi Tc-99m in vitro labeled RBC scan (Fig 8, Fig 9 and Fig 10). Describe the findings. The lesion does not demonstrate increased activity on 1 hour delayed blood pool imaging with Tc-99m labeled RBC.Ā The classic imaging findings of hemangioma on Tc-99m labeled RBC is initial photopenic area that slowly become visualized by 2 hours as the RBCs slowly replace the pooled blood in the dilated sinusoids. Filling may be uniform or progressive from peripheral to central. On delayed imaging the hemangioma is more intense in activity compared to the adjacent liver parenchyma. The one hour findings are not supportive for hemangioma in this study. The patient also underwent PET-CT as part of the initial staging of the disease. What are the expected FDG uptake patterns in hemangioma vs metastatic lesion? Cavernous hemangioma typically demonstrate low FDG uptake on PET. PET-CT is the most sensitive modality for detecting liver metastasis for many primary tumors (colorectal, lung, esophagus and breast). With regard to breast tumors, poor FDG uptake can be seen in lobular or tubular breast tumor. The axial PET images (Fig 11)Āand the fused images (Fig 12)Āshow the FDG uptake within the lesion is similar to blood pool. In this case of invasive ductal breast cancer, it is expected that metastatic lesion to the liver will demonstrate increased FDG uptake. ThisĀlesion was ultimately biopsied surgically and proven to be anĀhemangioma. |
| Diagnosis: Atypical Hemangioma |
| References:
Diagnostic Imaging Abdomen, Federle, Second Edition, AMIRSYS Hepatic Hemangioma: Atypical Appearances on CT, MR Imaging, and Sonography AJR 2003;180:135¢141 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 282077 The reader is fully responsible for confirming the accuracy of this content. |