|
| Patient: 31 year old male |
| History: 31 year-old man presenting to the emergency department with:
Cough and blood tinged sputum (2 weeks) Dypsnea (1 week) 3 pillow orthopnea (1 week) Paroxysmal nocturnal dyspnea
All of these symptoms have been intensifying over the past 2 days
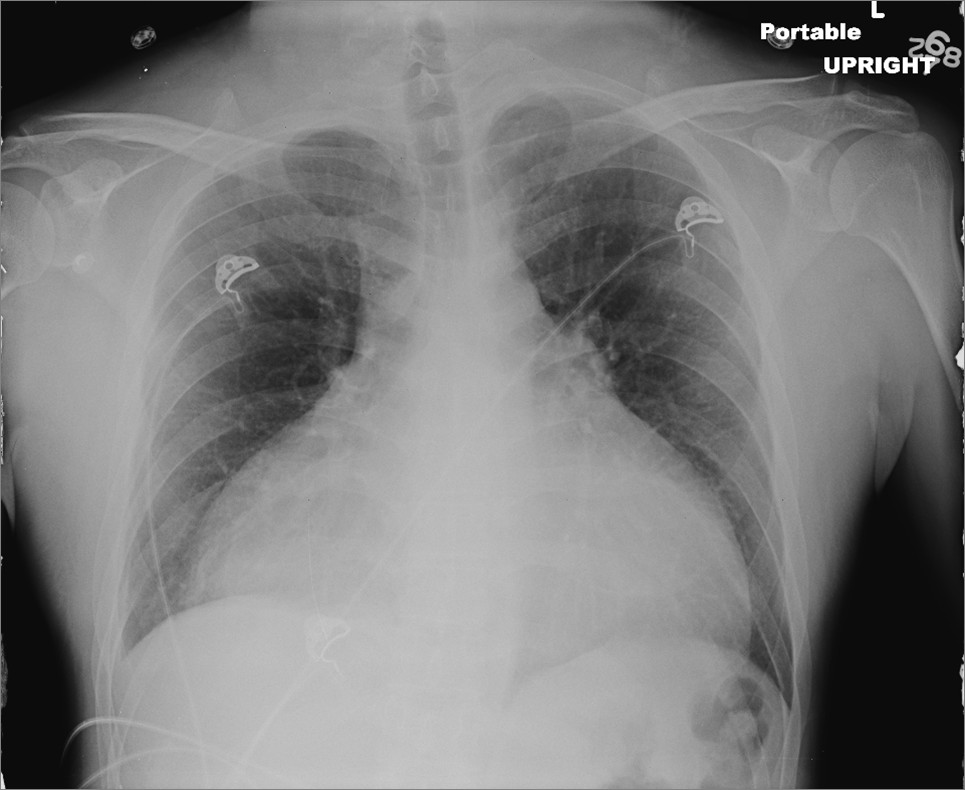
Chest radiograph on presentation
Figure 1
Interpretation?
Echocardiogram after pericardial drainage
Figure 2: 4 Chamber Figure 3: 4 Chamber Doppler (MV plane) Figure 4: RVOT Figure 5: RVOT Doppler
Interpretation?
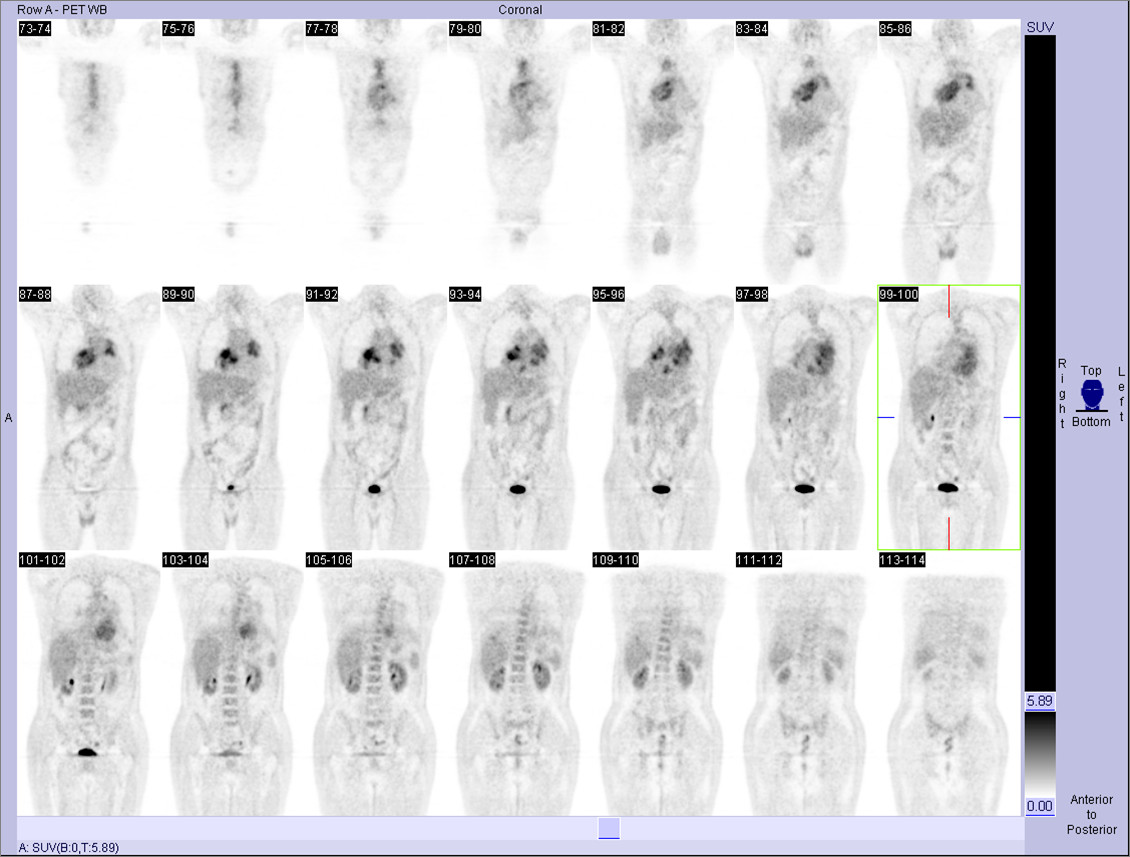
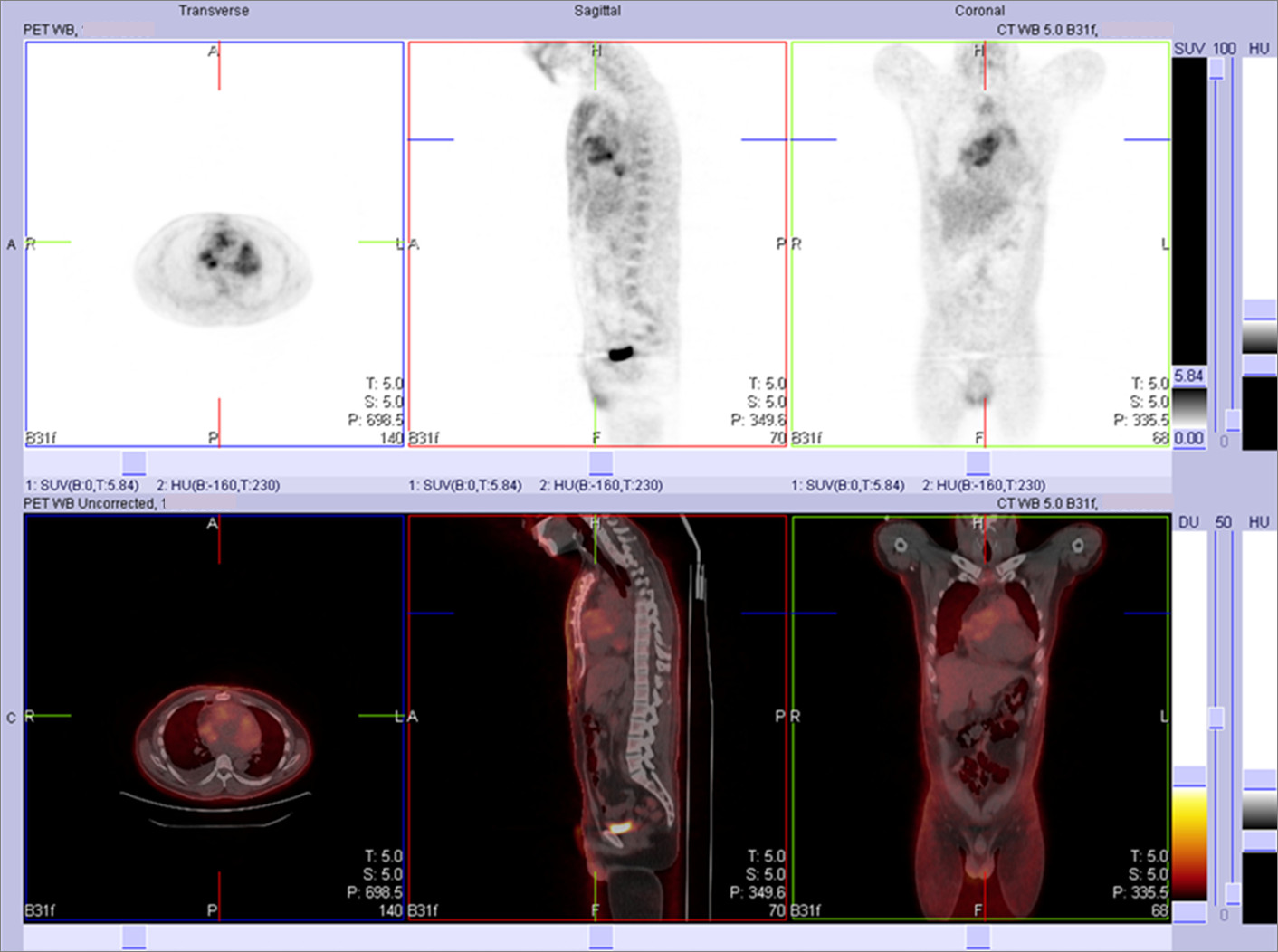
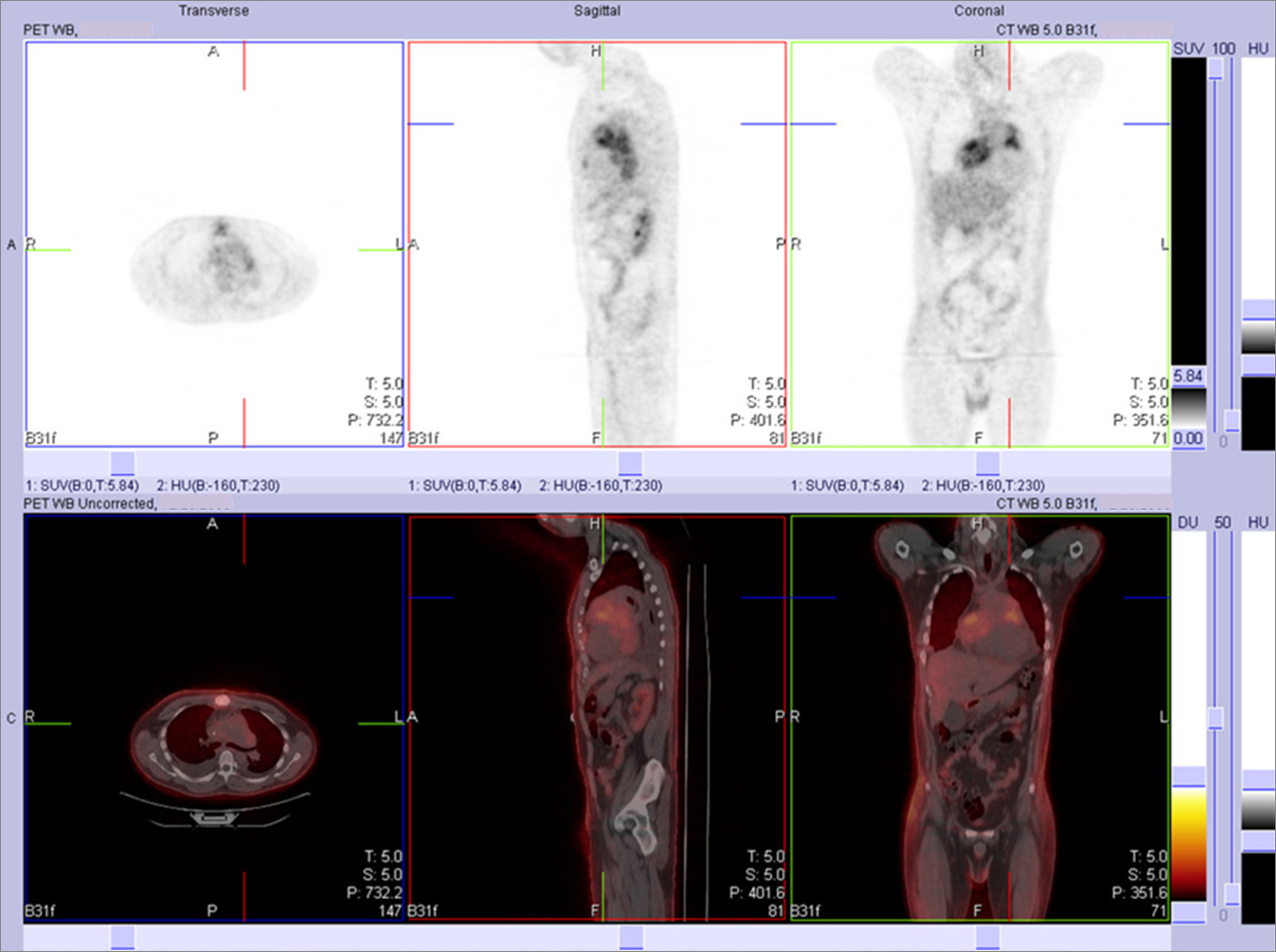
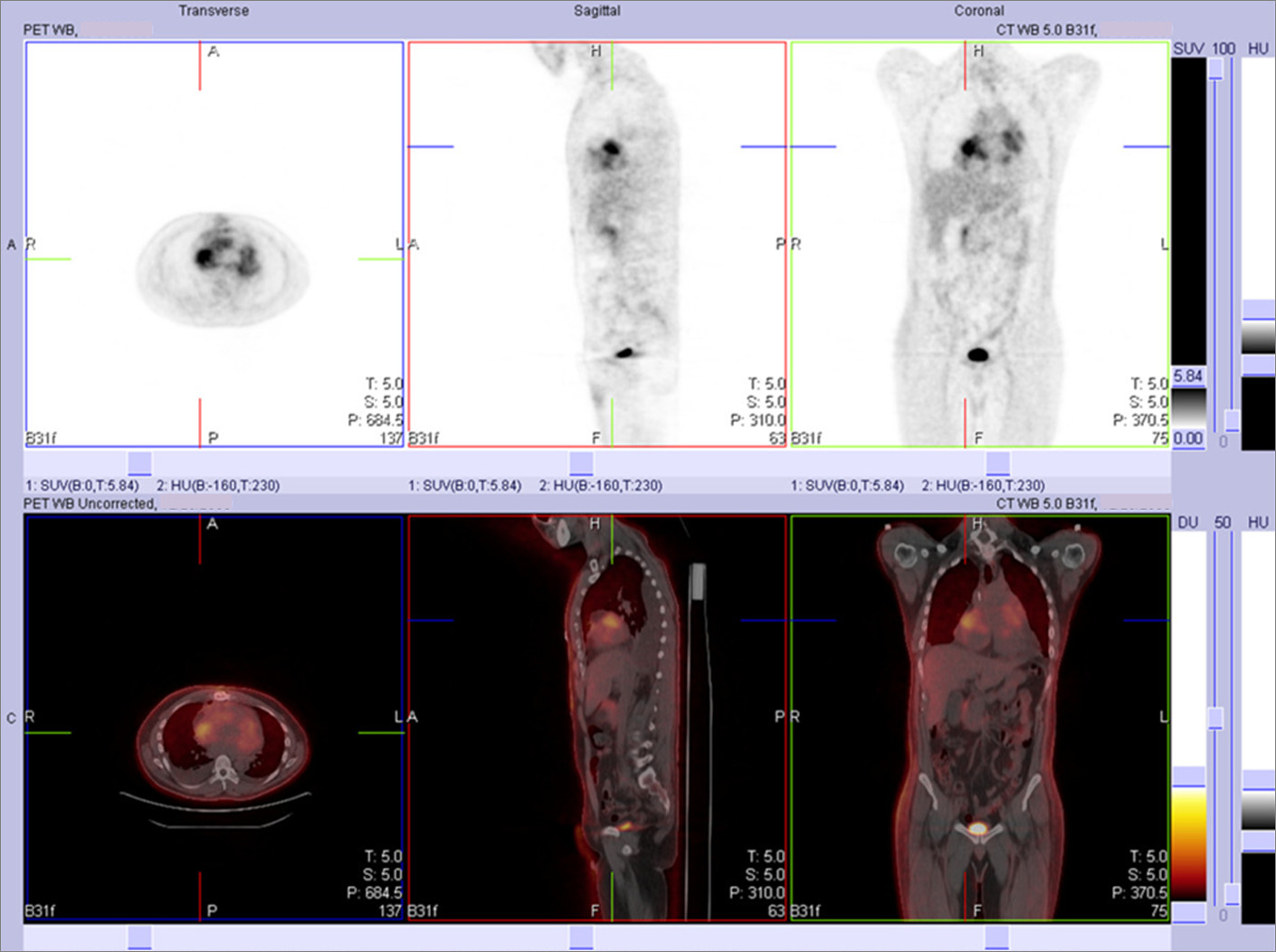
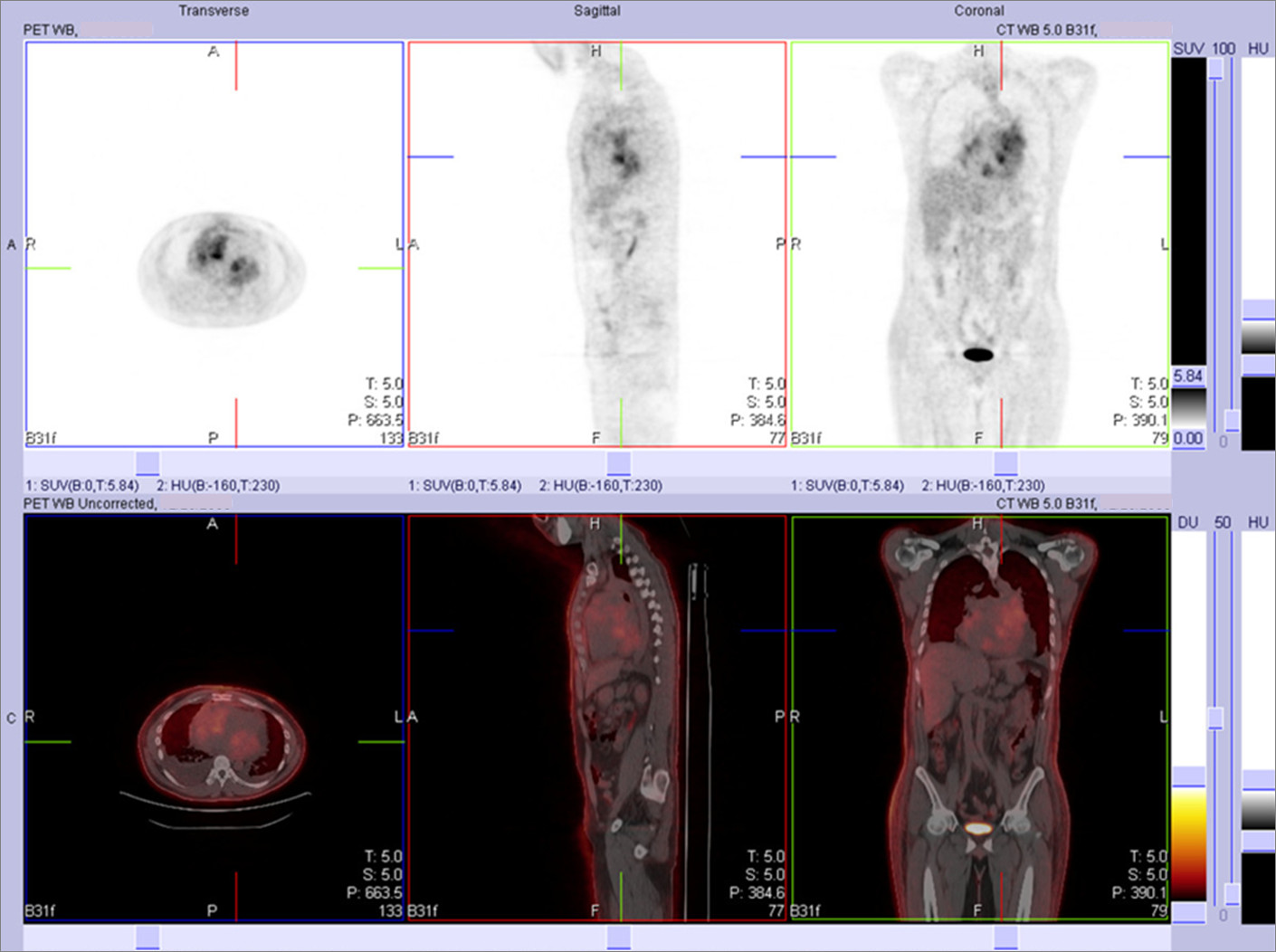
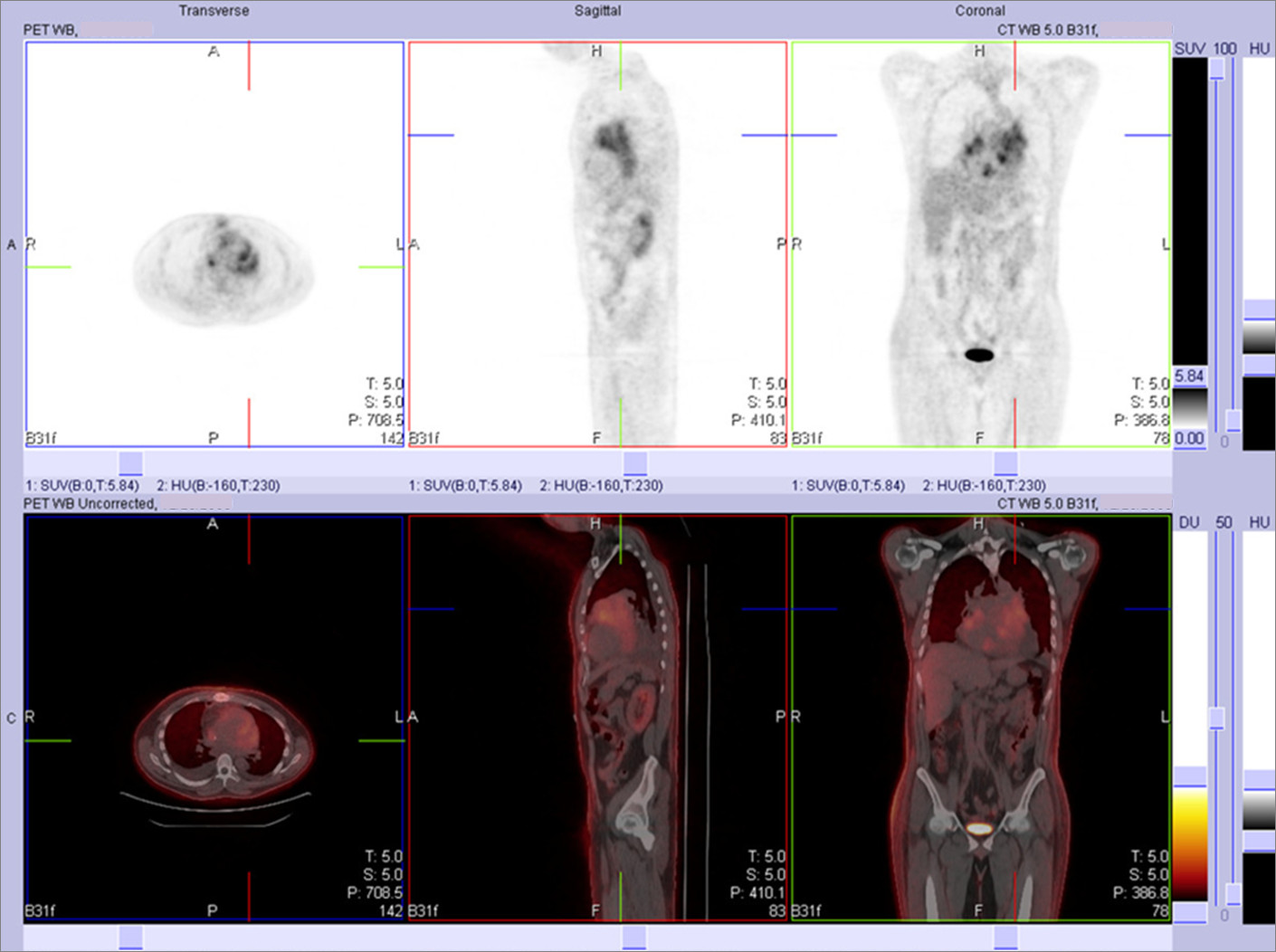
What nuclear medicine study may be helpful?
Figure 6 Figure 7 Figure 8 Figure 9 Figure 10 Figure 11 Figure 12 Figure 13
Interpretation and next step in management?
|
Image Size:
|
| Findings: Frontal Chest Radiograph: Ā Marked enlargement of the cardiac silhouette.ĀĀIf this finding is acute, these findings may be due to a pericardial effusion. Echocardiography can be performed for further evaluation.Ā Otherwise, consider ischemic cardiomyopathy, anomalous coronary artery from pulmonary artery, or adjacent mediastinal opacity (such pericardial cyst/lymph node/mass). Ā Echocardiogram: Ā Multiple intracardiac masses of different sizes and shapes in the right atrium, main pulmonary artery, left atrium, and superior left pulmonary vein.Ā The largest of these is in the left atrium, measures 3.5 cm x 3 cm, and prolapses into the left ventricle during systole.Ā A massive pericardial effusion is present without hemodynamic compromise.Ā Ā PET-CT: RADIOPHARMACEUTICAL: 13.9 mCi F-18 Fluorodeoxyglucose (FDG) i.v. There are abnormally hypermetabolic masses of varying shapes and sizes involving the right atrium, left atrium, left atrial appendage with extension to the left upper pulmonary vein, and main pulmonary artery. A moderate sized pericardial effusion is present and there is a single focus of increased activity in the anterior pericardial space adjacent to the sternum, at table position 690, which may represent extracardiac extension of one of the cardiac masses. No additional foci of abnormally increased FDG uptake noted throughout the rest of the body to suggest extrathoracic disease. Ā There is mildly increased uptake along the median sternotomy site, postsurgical in nature. Several mildly prominent abdominal para-aortic lymph nodes are present demonstrating FDG uptake less than blood pool. These lymph nodes are likely reactive in nature. Ā Additional findings on the noncontrast CT portion study include a large right pleural effusion and a small left pleural effusion. There is associated compressive atelectasis, right greater than left. Both pleural effusions do not demonstrate increased FDG uptake. A right subclavian approach port is in place with its tip near the cavoatrial junction. There is a small amount of air in the pericardial sac likely from recent pericardiocentesis. The gallbladder is moderately distended. Diffuse body wall edema is noted. |
| DDx: Primary Cardiac Tumors (benign and malignant) Ā Myxomas Ā Sarcomas Ā Others (leiomyoma, rhabdomyoma, fibroma, lipoma) Ā Metastasis Ā Lymphoma (Primary or Systemic) |
| Diagnosis: Primary cardiac B-cell lymphoma |
| References: https://my.statdx.com |
| Comments: No comments posted. |
| Additional Details:
Case Number: 245546 The reader is fully responsible for confirming the accuracy of this content. |