General Discussion: Full Patient History:
The patient is a 19-month-old infant girl with idiopathic infantile spasms and refractory seizures. The patient experienced a seizure approximately 33 minutes into the uptake phase of the FDG-PET study.
General Discussion:
Epilepsy intractable to multiple medications requires evaluation for surgical treatment. This evaluation typically includes video monitored electroencephalogram (video-EEG), and FDG-PET and/or cerebral perfusion SPECT studies.
In this case, the infant patient was diagnosed with infantile spasm, age-dependent myoclonic seizures that occur with an incidence of 25:100,000. The most common causes are congenital malformations, perinatal asphyxia, and tuberous sclerosis. It can also be part of Aicardi syndrome, along with agenesis of corpus callosum and retinal malformation. Her brain MRI did not reveal any abnormality. Hence FDG-PET study was performed in hope for identifying an epileptogenic focus for intervention.
FDG-PET study is used to evaluate metabolic activity of the brain, specifically the cortices and subcortical nuclei, only during the interictal state. Immature normal brain typically demonstrates hypermetabolism in bilateral sensorimotor cortex, thalami, and cerebellar vermis. By 1 year of age, a normal infant has FDG uptake pattern resembling that of a normal adult.
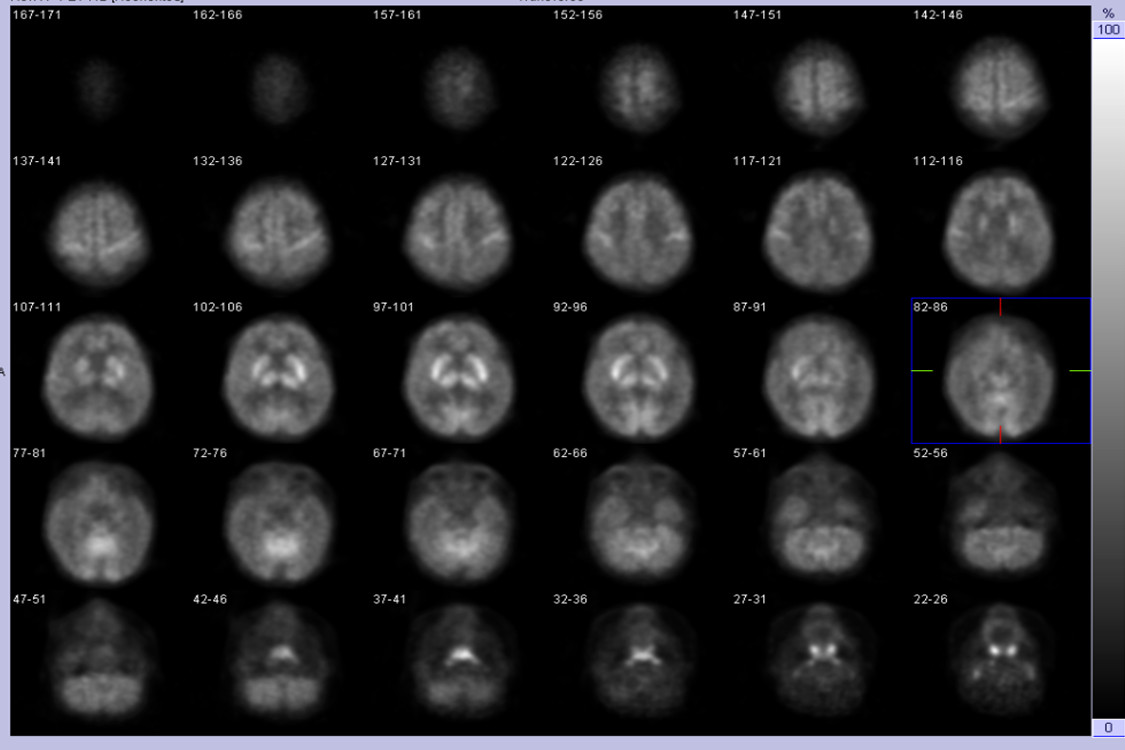
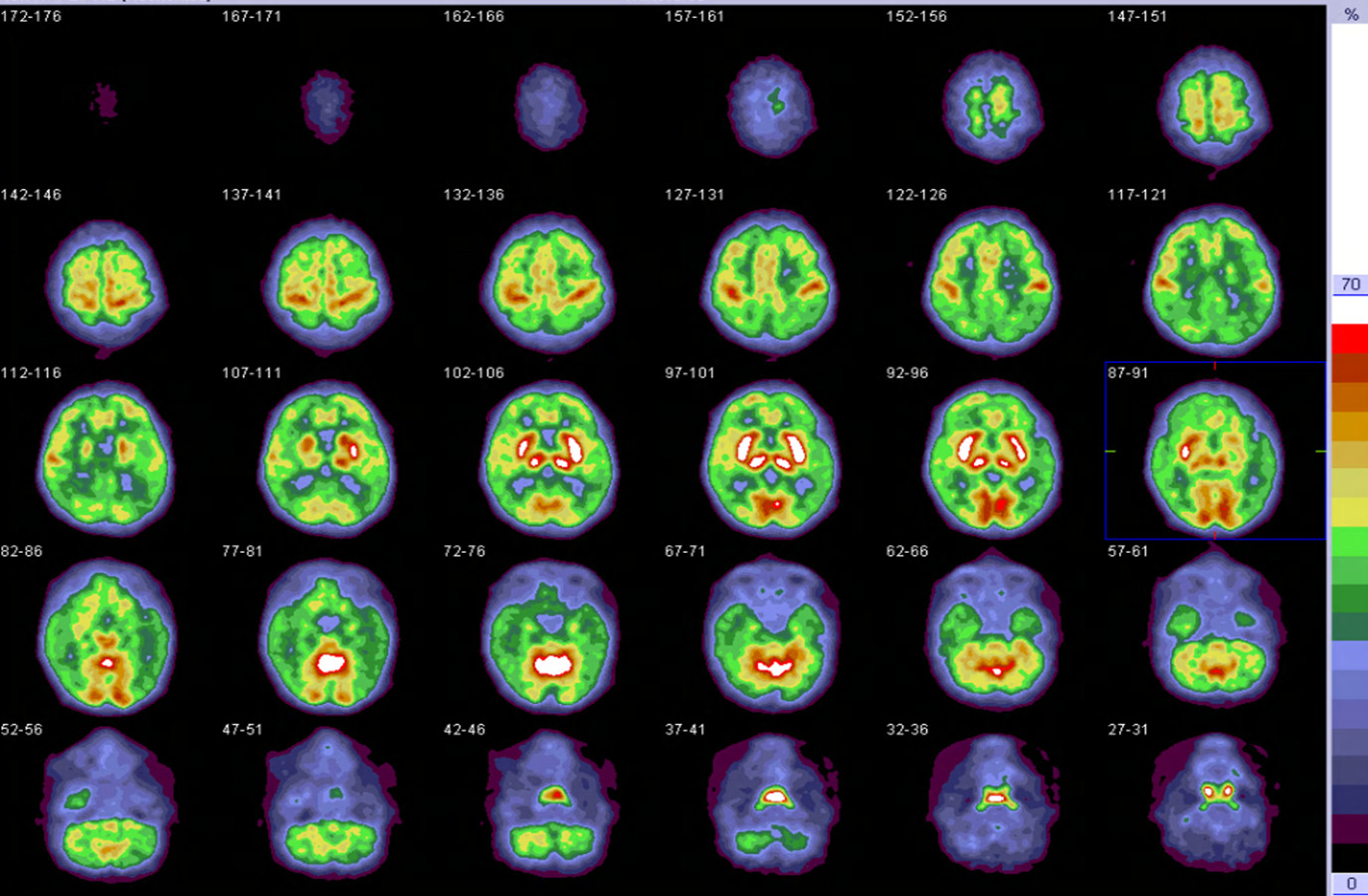
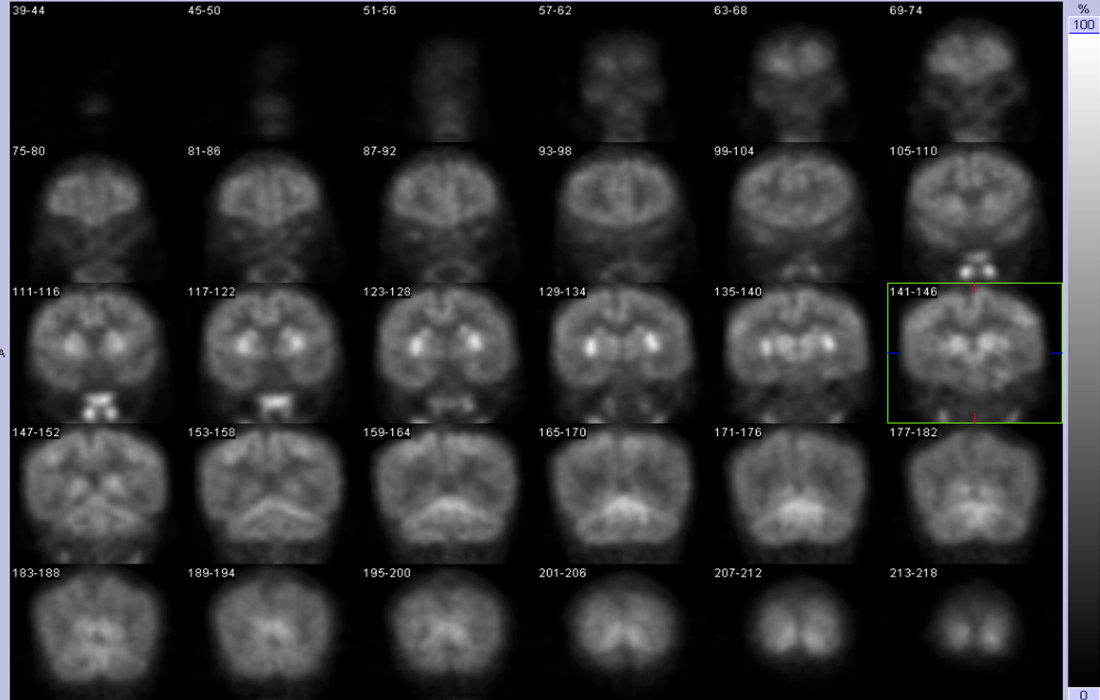
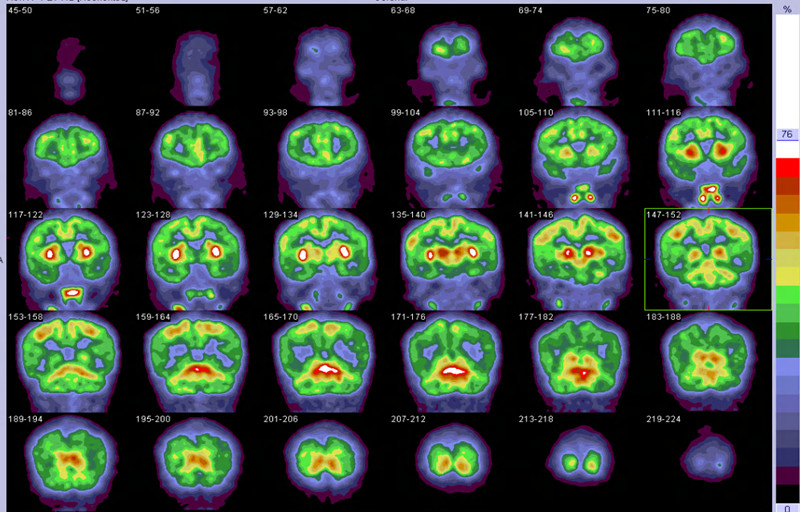
As this case demonstrates, ictal FDG-PET is not useful because the long uptake phase covers the entire ictal event and extends into the postictal state. The resultant image would not be true representation of the initial phase of an ictal state, where the epileptogenic location might be identified as a hypermetabolic focus. This study was intended to capture the interictal state. Due to high frequency of this patient’s seizures, an incidental seizure occurred 33 minutes after radiophamaceutical injection, well into the uptake phase. The seizure activity yield this study nondiagnostic, as hypermetabolic areas likely represent spread of seizure activity, rather than true epileptogenic sites (Figure 1, Figure 2, Figure 3, and Figure 4).
In the interictal state, epileptogenic focus is known to be hypometabolic in the interictal state, and hypermetabolic in the ictal state. Hence, on an interictal FDG-PET study, focal hypometabolism in the cerebral cortex is interpreted as potential epileptogenic focus, unless any abnormality is identified on brain MRI to explain this finding. Hypometabolic area related to an epileptogenic focus can be much larger than the focus itself, as it represents area affected by the seizure focus, and not just the focus itself. Therefore, often the study is clinically useful only to demonstrate which side the seizure might be coming from (lateralization), rather than the exact epileptogenic focus. The sensitivity for identifying lateralization is about 70%.