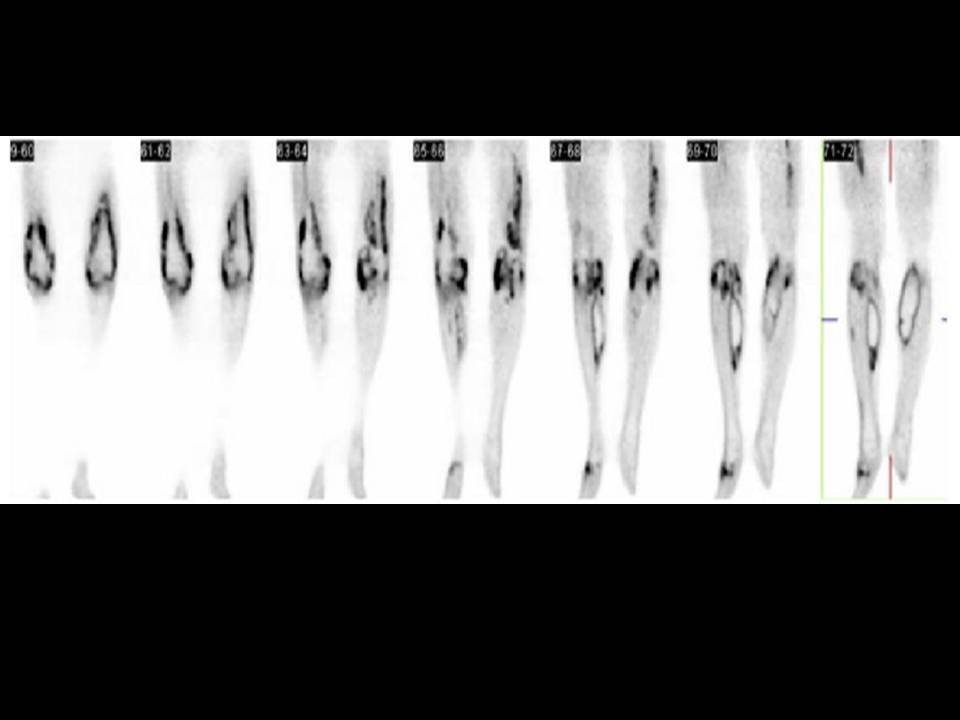
General Discussion: Radiopharmaceutical: 13.2 mCi F-18 Fluorodeoxyglucose i.v.
Long History history: This is a 55-year-old woman who was in her usual state of good health until approximately 1-1/2 weeks ago when she developed fever, back pain, and symptoms of malaise and an upper respiratory infection. She presented to her primary physician who prescribed non-steroidal anti-inflammatory medications. She subsequently developed severe joint pain of the lower extremities and bilateral leg swelling. She is on no other medications and reports no history of malignancy. The patient was admitted for further evaluation. A chest CT was acquired that demonstrated numerous subcentimeter indeterminate pulmonary nodules in both lungs that were concerning for pulmonary metastases of an unknown primary.
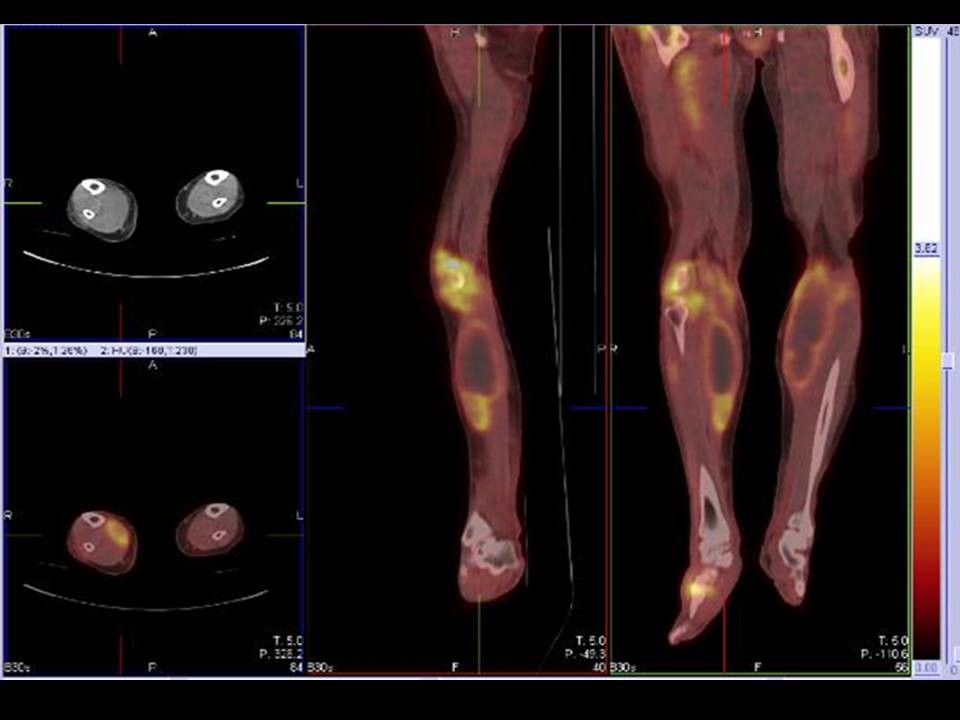
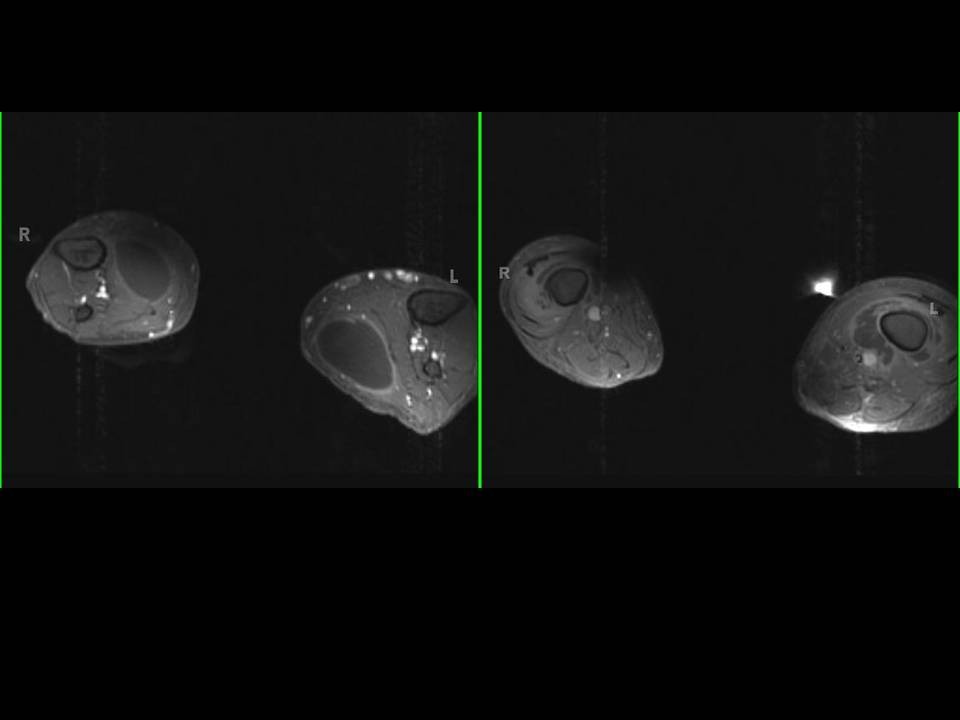
Discussion: Pyomyositis, a purulent infection of skeletal muscle that is usually caused by Staphylococcus aureus.Once considered a tropical disease, it is now seen in temperate climates as well, particularly with the emergence of HIV infection. In addition to HIV, other viruses, bacteria (including mycobacteria), fungi, and parasites can cause myositis. Single or multiple muscle groups in the limbs can be involved. MRI is helpful in differentiating pyomyositis from osteomyelitis. FDG-PET is non-specific and complementay to CT or MRI for diagnosis pyomyositis.
Follow up:ĀĀcytology of right calf muscle demonstrated cellular debris and acute inflammation.ĀBlood culture was positive forĀSTAPHYLOCOCCUS AUREUS. he underwent I&D of the bilateral calf muscles, collections as well as arthroplasty and I&D of her
bilateral septic knee joints. Evaluation for endocarditis which was the presumed origin given her multiple distal abscesses revealed no echocardiographic evidence of vegetation on her heart valves by transthoracic echocardiogram.Ā Cardiac Echo demonstrated right to left shunt. Patient was treated Oxacillin for presumed bacterialĀendocarditisĀand discharge home.