General Discussion: FULL PATIENT HISTORY : 35-year-old Caucasian woman with a history of end-stage
renal disease secondary to reflux nephropathy status post first renal
transplant in 2000 with subsequent failure in May 2007 for unclear reasons,
possibly BK virus, status post second renal transplant in July of 2007. She
was found to have CMV viremia with a viral count of 400,000 in her blood in December 2007. She was then treated with high-dose valganciclovir. However, she
developed fevers, chills, drenching night sweats, and iliosacral pain. The
patient was admitted to the hospital and it was thought that her
symptoms may have been from the valganciclovir. However, since her symptoms
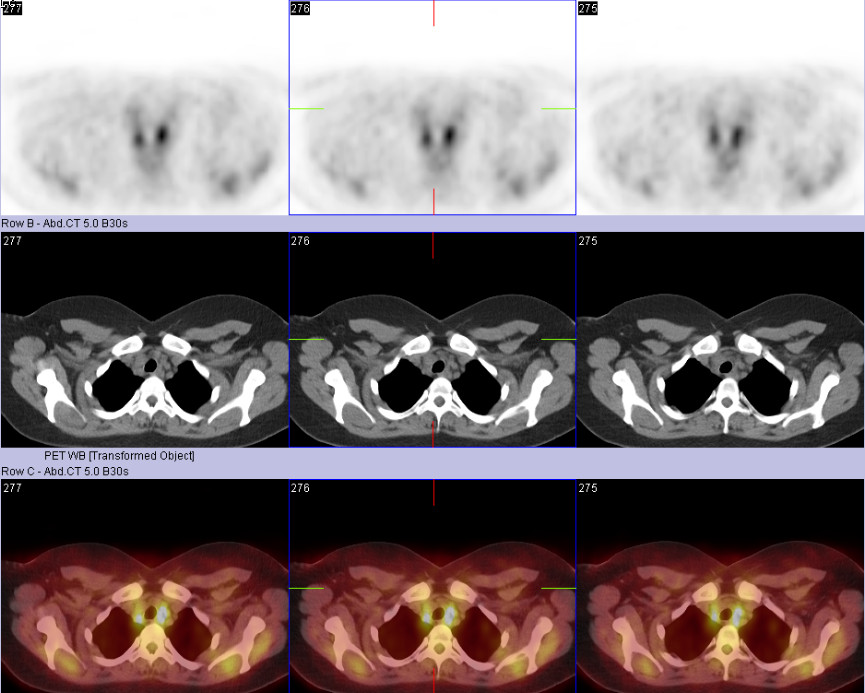
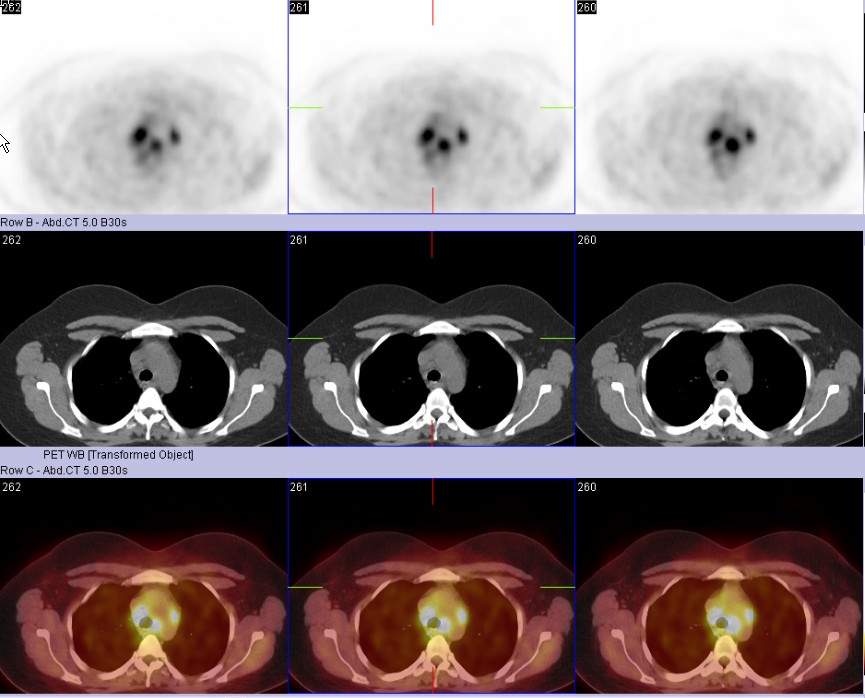
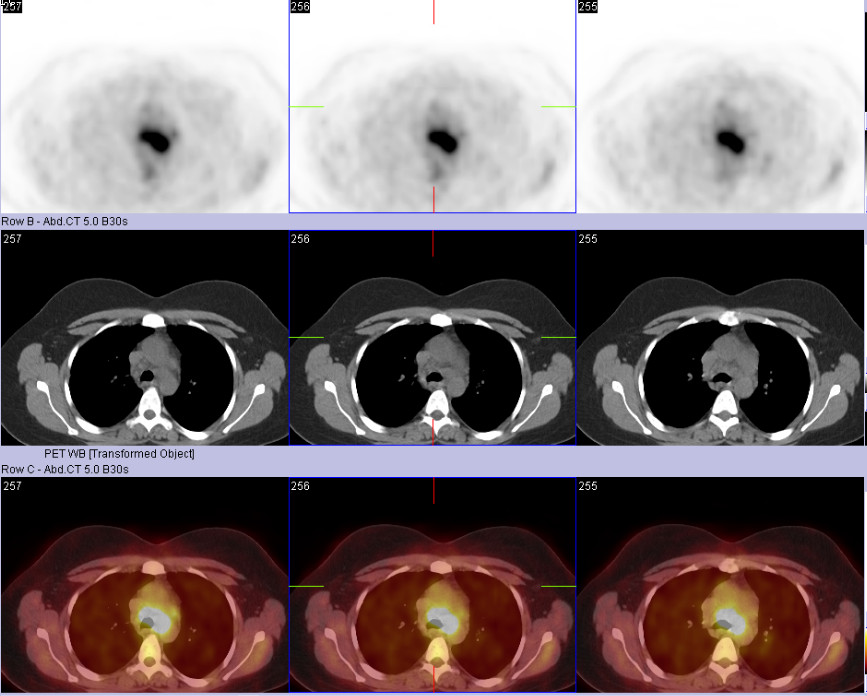
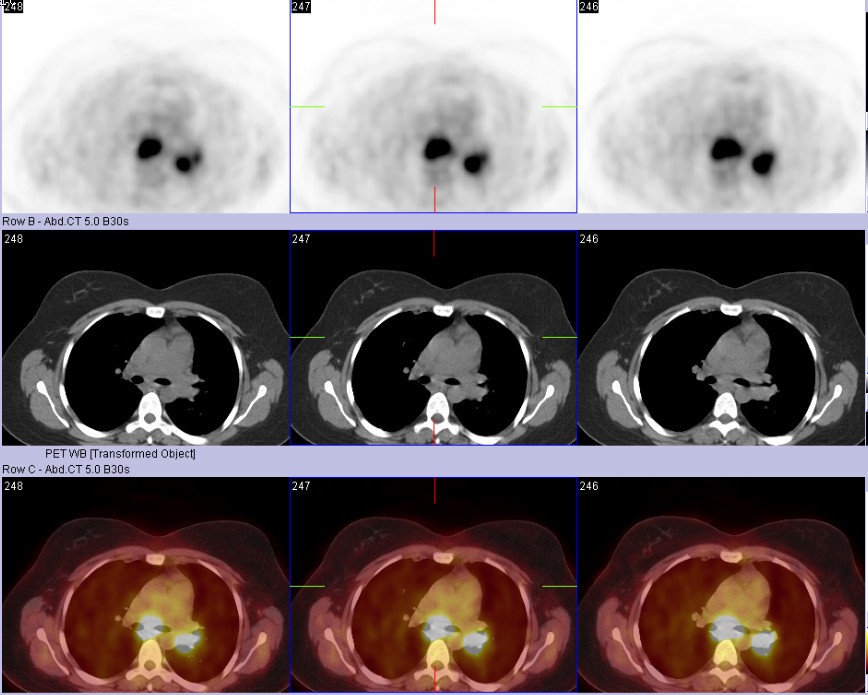
were concerning for lymphoma, she underwent total body PET-CT scan which
revealed mediastinal lymphadenopathy (right paratracheal, para-aortic,
prevascular, aortopulmonary, subcarinal, and left hilar lymph nodes) which had
increased FDG uptake that was suggestive of lymphoproliferative disease (PTLD).
She then underwent lymph node biopsy by mediastinoscopy which revealed
histoplasma capsulatum on microbiology staining. Pathology also revealed
granulomatous lymph-adenitis with fungal organisms and so the patient was
diagnosed with Histoplasmosis and she has been started on itraconazole, 200
milligrams t.i.d.
DISCUSSION : In this post renal transplant patient presenting with fever, chills and drenching night sweats, a post transplant lymphoproliferative disorder is the most likely diagnosis, given the extensive FDG avid mediastinal lymphadenopathy seen on the PET study. However, it is important to include other infectious causes like histoplasmosis in the differential. The patient was status post transplant and was on multidrug immunosuppressive therapy, making her susceptible to fungal infections.
Histoplasmosis is the most common of the endemic mycoses and a major cause of morbidity and mortality in patients living in endemic areas like ours.The respiratory tract is considered the portal of entry for H capsulatum in most patients. Cellular immunity plays the primary role in defense against the organism.
The clinical spectrum of the disease depends on the extent of exposure, age, presence of underlying lung disease, general immune status, and specific immunity to H capsulatum. Lungs are the most common organs involved. Infections can be classified as follows:
Pulmonary histoplasmosis - Acute asymptomatic pulmonary histoplasmosis: This is the most common manifestation that occurs following histoplasmosis infection (>90%). This type commonly occurs in individuals with normal immunity residing in endemic areas.
- Acute symptomatic pulmonary histoplasmosis: This is a benign, self-limited illness characterized by symptoms of fever, chills, headache, cough, and retrosternal or pleuritic chest pain. Malaise, weakness, fatigue, and myalgia are observed in a distinctly smaller percentage of patients. Symptoms commonly are mistaken for a flulike illness; however, coryza and sore throat are not typical symptoms of histoplasmosis and suggest alternative diagnoses. Acute reinfection pulmonary histoplasmosis: This is not uncommon in those residing in endemic areas and subject to reexposure. The duration of illness is often shorter than it is in primary infection. The characteristic chest radiograph shows numerous small nodules diffusely scattered throughout both lung fields.
- Chronic pulmonary histoplasmosis: This occurs in patients with underlying lung disease, especially chronic obstructive pulmonary disease (COPD).
- Progressive disseminated histoplasmosis (PDH): It occurs in immunodeficient patients with defective T-cell immunity (patients with AIDS or hematologic malignancies [eg, Hodgkin and non-Hodgkin lymphoma] or those taking immunosuppressive medications). Patients at the extreme of ages also are at risk for disseminated disease. PDH can develop upon reexposure to a large inoculum of the fungus or upon reactivation of dormant endogenous foci. Most cases are believed to arise from endogenous reactivation, because the disease develops in those who reside in remote endemic areas. Fever and malaise are the 2 most common manifestations, followed by weight loss, cough, and diarrhea. Patients can develop hepatosplenomegaly, lytic bone lesions, skin lesions, peripheral lymphadenopathy, prostatitis, or epididymitis.
Miliary pulmonary histoplasmosis: This is a special presentation that follows a more intense exposure. Patients often develop reticulonodular or miliary pulmonary infiltrates (a scenario that resembles miliary tuberculosis) and may progress to respiratory failure or extrapulmonary PDH Nonpulmonary histoplasmosis -Pericarditis .
-Rheumatologic syndromes, such as arthralgias, erythema nodosum, and erythema multiforme, are present in approximately 6% of patients, most of whom are women. In some patients, this manifestation of histoplasmosis may be the presenting complaint. Frank arthritis is distinctly uncommon.
-Sarcoidosis-like syndrome is so termed because distinguishing between histoplasmosis and sarcoidosis can be difficult. The 2 disorders may demonstrate similar histopathologic features, and serum angiotensin-converting enzyme levels are elevated in both. Therefore, for patients presenting with mediastinal or hilar lymphadenopathy and residing, or having recently resided, in an endemic region, it is critically important to consider histoplasmosis in the differential diagnosis.