|
| Patient: 58 year old female |
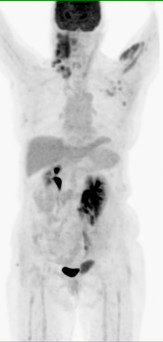
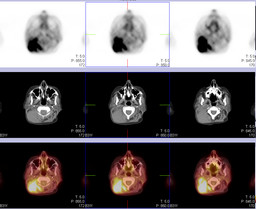
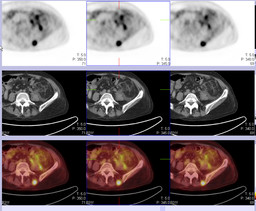
| History: 50-year-old woman with acute myeloid leukemia, treated with stem cell transplant. A recent biopsy of a right neck mass demonstrated myeloid sarcoma.PET-CT was requested to stage the disease. |
Image Size:
|
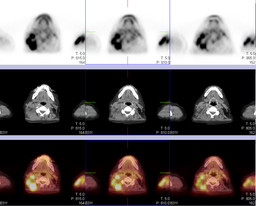
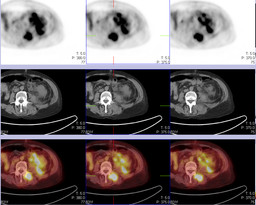
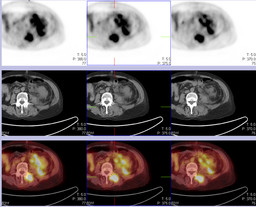
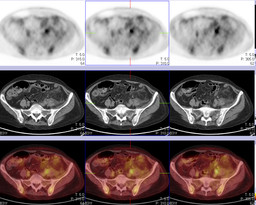
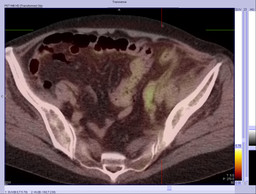
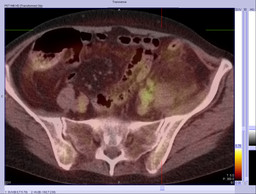
| Findings: FDG-PET: There is a large soft tissue mass in the posterior right neck, representing a conglomerate of There are also foci of increased FDG uptake within the lower abdomen and pelvis along the course of the left ureter, most consistent with iliac chain lymph node deposits. The proximal left ureter is dilated, and there is left hydronephrosis. In addition, inflammatory stranding and free fluid surround the left kidney; there is extrarenal extravasation of FDG into the retroperitoneum, from forniceal rupture. Impression: Extensive metabolically active soft tissue deposits representing myeloid sarcoma within the neck, left upper extremity, abdominal wall, lumbar paraspinal muscles, and left iliac chain lymph nodes, the latter of which caused left-sided hydroureteronephrosis and forniceal rupture.
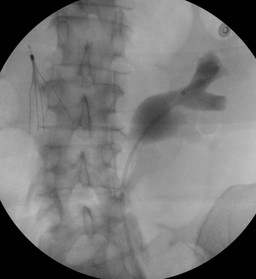
Left sided retrograde pyelogram followed by stent placement was performed.
|
| DDx: 1.Extensive metastases from known myeloid sarcoma. Acute left ureteric obstruction with calyceal rupture. |
| Diagnosis: Acute calyceal rupture due to acute left distal ureteric obstruction by enlarged metastatic lymph nodes. |
| References: 1.Gennaro Cormio, M.D., Luigi Cormio, M.D., Ph.D.,*,1 Giuseppe Di Gesu’, M.D., Giuseppe Loverro, M.D.,and Luigi Selvaggi, M.D. CASE REPORT: Calyceal Rupture and Perirenal Urinoma as a Presenting Sign of Recurrent Ovarian Cancer; Gynecologic Oncology 83, 415–417 (2001) 2.Phornthep Ruchdaphornkul, Kamol Panumatrassamee; Clinical report:Transitional cell carcinoma of ureter presenting acute ureteric colic and ruptured caliceal fornix with extravasation of urine; Asian Biomedicine Vol. 4 No. 6 December 2010; 935-938. 3.Eric J. Heffernan and Stephen J. Skehan;INTERESTING IMAGE: Calyceal Rupture Secondary to Ureteric Obstruction by recurrent Colorectal Carcinoma; Clin Nucl Med 2007;32: 199–200. 4.http://emedicine.medscape.com/article/382530-overview#a23 5.Boris Gershman, Naveen Kulkarni, Dushyant V. Sahani and Brian H. Eisner; Causes of renal forniceal rupture; 2011 BJU INT ERNATIONAL |
| Comments: No comments posted. |
| Additional Details:
Case Number: 326971 The reader is fully responsible for confirming the accuracy of this content. |