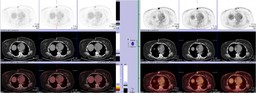
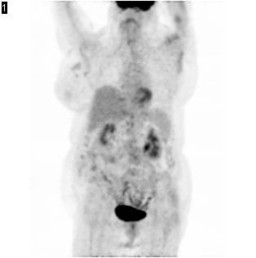
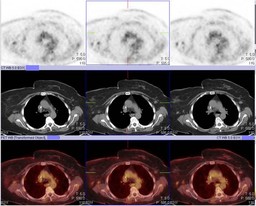
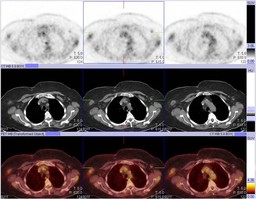
General Discussion: ĀIn light of the PET estradiol challenge test, the treatment plan was changed to chemotherapy. The patient underwent a PET study(PET 3) after completion of chemotherapy which showed marked response to therapy.
Most breast cancers are estrogen receptor (ER)-positive (ER+) tumors and therefore potentially hormone responsive. Despite this, chemotherapy often is chosen over hormonal therapy in the initial management of advanced breast cancer, at least in part because many physicians believe that chemotherapy is more likely to produce tumor shrinkage and to produce it more rapidly than hormonal agents. Even in elderly women, who tend to have a more indolent disease process, it has been reported that hormonal therapy is underused.In advanced ER+ breast cancer, the likelihood of response to hormonal therapy is equivalent to the likelihood of response to chemotherapy.
Hormonal therapies are consistently underused in the management of breast cancer, although the majority of patients have ER+ disease.The presence of ER alone predicts clinical benefit in 55% to 60% of patients. If both ER and PR are present, the likelihood of benefit increases only slightly, to 60% to 70%.The presence of a hormone receptor does not indicate that the receptor is functional and essential to the growth of the cancer cell, of course, nor does it imply that interference with receptor function will result in tumor-cell kill. None of the available serologies, prognostic factors, or radiologic studies can accurately predict for clinical benefit from hormonal therapy.
Hormone flare reactions seem to be more predictive of hormone responsiveness than the results of receptor assays, because flare indicates that the receptors are both present and functional. The flare reaction typically occurs in postmenopausal women with ER+ breast cancer and osseous metastases. Within 7 to 10 days of initiation of hormonal therapy, patients develop increased pain at metastatic sites, often accompanied by increased serum calcium, alkaline phosphatase, or tumor markers.Serial skeletal scintigraphy may show increased activity at sites of known metastasis or may identify areas not appreciated on pretreatment scintigrams. Although this clinical presentation often is indistinguishable from disease progression, true hormone-induced flare reactions herald subsequent response to treatment in 75% to 90% of patients. Nevertheless, clinical flare is of limited use in the prediction of response because it is uncommon (observed in less than 5% of patients), although it may occur at a subclinical level in more patients.
In patients with functional ER, metabolic flare can be seen following treatment with tamoxifen or after short treatment with estradiol.