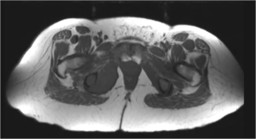
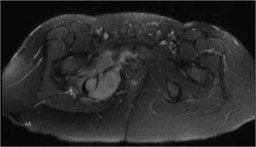
General Discussion: The patient first presented to the ER with severe right hip pain radiating down her thigh. Plain films of the pelvis showed no abnormality. The patient subsequently underwent an MR which showed a 6.1 centimeter mass of the right ischium destroying the
cortex. Subsequent imaging showed widespread metastatic disease. The patient was initiated on palliative radiation
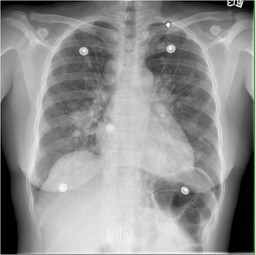
therapy. She was also treated for newly diagnosed large bilateral pulmonary emboli, as well as, a hospital-acquired pneumonia. Despite therapy, her cancer was highly aggressive.The patient expired five months after presenting to the ER with hip pain.
Melanoma is a malignancy of pigment-producing cells (melanocytes) located predominantly in the skin, but also found in the eyes, ears, GI tract, leptomeninges, and oral and genital mucous membranes. Malignant melanoma accounts for 4% of all skin cancers, but it causes 79% of skin cancer deaths. The incidence of melanoma has more than tripled in the white population during the last 20 years, and melanoma currently is the sixth most common cancer in the United States
Malignant melanoma is not a common cause of cancer metastasis to the skeleton. However, when melanoma does metastasize, one of the most common sites is the skeleton.
Melanoma is categorized in four stages by the American Joint Committee on Cancer. Stage I has a Breslow depth of less than 2.01 mm and no ulceration; stage II has a Breslow depth of greater than 2.0 mm or lesions at 1.01 - 2.0 mm in depth with ulceration; stage III has regional lymph node metastasis; and stage IV has distant metastasis, which may include metastasis to bone. Autopsy studies indicate 23-49% osseus inlvolvement in patients who die from malignat melanoma. The mean survival time for patients with skeletal metastasis from malignant melanoma ranges from 3.6-4.7 months
Osseous metastases may remain invisible on plain films until cortical destruction has occurred, and scintigraphy may miss those lesions that are growing either too aggressively or too slowly to incite significant reactive bone formation.