|
| Patient: 55 year old male |
| History: HISTORY: 55-year-old man with multiple myeloma with associated spinal plasmacytoma and cord compression status post chemotherapy and radiation. |
Image Size:
|
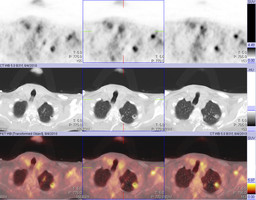
| Findings: RADIOPHARMACEUTICAL: 15.0 mCi F-18 Fluorodeoxyglucose (FDG) i.v.
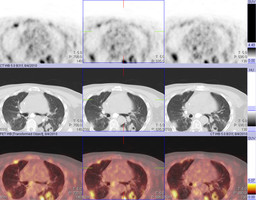
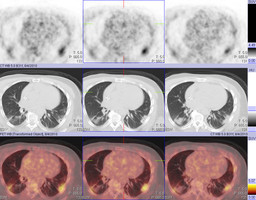
FINDINGS: There are multiple bilateral pulmonary nodules/masses. There is a 3.0 x 1.0 cm mass within the left apex with moderately increased FDG uptake. There is a 1.5 x 2.0 cm cavitary nodule within the left upper lobe with moderately increased FDG uptake. There is a 3.8 x 2.6 cm cavitary mass within the left lower lobe with mild to moderate increased FDG uptake about the periphery. There are numerous bilateral pleural based soft tissue masses with moderately increased FDG uptake.
ADDITIONAL FINDINGS (not pertinent to the major teaching point): There is diffuse, severe, and destructive osteolytic disease throughout the visualized skeleton. The majority of these osteolytic lesions demonstrate abnormal FDG uptake, although there are some osteolytic lesions, predominantly within the pelvis which do not demonstrate abnormally increased FDG uptake. Note there is extension into the spinal canal at the T4 level. There is diffuse thickening of the cecum with associated mild increased FDG uptake. Pericecal inflammatory stranding is noted. There is a moderate amount of free fluid about the right lower quadrant. |
| Diagnosis: 1. Multiple bilateral hypermetabolic pulmonary and pleural nodules/masses, some of which are cavitary. Multiple cavitary hypermetabolic pulmonary nodules could be the sequela of septic emboli.Ā Differential diagnosis also includes Wegener's granulomatosis and metastatic disease. Ā 2. Diffuse, severe, and destructive osteolytic disease throughout the visualized skeleton, most of which is hypermetabolic. There are some foci without abnormally increased FDG uptake which may represent fibrosis of the marrow with treated disease. Ā 3. Diffuse cecal thickening with mild increased FDG uptake with pericecal inflammatory stranding, moderate amount of free pelvic fluid and questionable extraluminal gas. Findings are likely of an inflammatory nature. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 297014 The reader is fully responsible for confirming the accuracy of this content. |