| Findings: PET-CT:
Radiopharmceutical: 9.9 mCi F-18 Fluorodeoxyglucose i.v.
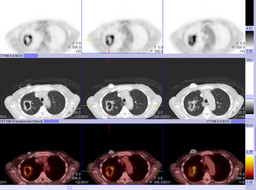
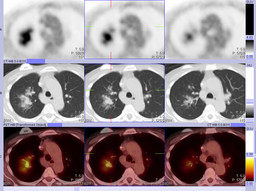
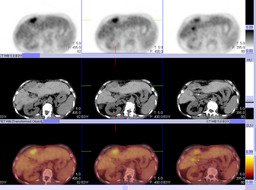
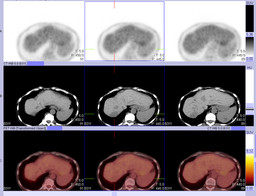
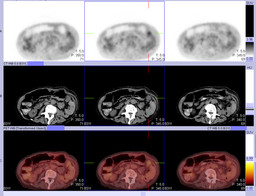
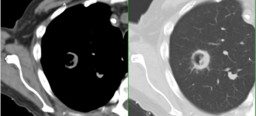
There has been significant interval increase in size of the right upper lobe cavitary lesion. This demonstrates a thick, intensely FDG-avid rim with surrounding groundglass attenuation and nodular consolidation (Figure 2). The maximal SUV is increased from 4.4 to 6.4 (prior PET-CT not shown). This is most consistent with a progressive infectious process such as a fungal infection. New nodular groundglass opacities are noted in the right perihilar lung (Figure 3). These demonstrate mild FDG uptake and likely represent spread of infection. Small nodules within the left upper lobe along the major fissure and in the right base have decreased in size when compared with the prior study. No associated FDG uptake is appreciated in these nodules; however, these are below the resolution of PET. There are multiple low attenuation lesions in the peripheral aspect of segment 4B of the liver. The largest lesion has unchanged FDG uptake (Figure 4); however, it has decreased slightly in size compared with the prior study. The remaining lesions demonstrate FDG uptake comparable to the surrounding liver (not shown). There is unchanged, persistent intense FDG uptake in the region of the liver hilum (Figure 4). This may be within the liver, within a hilar lymph node, or within the duodenum. A lobulated peritoneal mass in the left upper quadrant is unchanged in size and degree of mild FDG uptake (Figure 5 and Figure 6). Again seen is a low attenuation lesion in the spleen which shows mildly greater FDG uptake in the surrounding spleen, also unchanged (Figure 5). Noncontrast CT images demonstrate postsurgical changes of left nephrectomy and partial colectomy with colocolonic anastomosis. Embolization coils are seen in the right hepatic and gastroduodenal arteries. There is associated atrophy of the right hepatic lobe. There is high attenuation material within low attenuation hepatic lesions in the liver dome and in segment 8, consistent with prior embolization. Chest CT (2 months before PET-CT):
There has a new 2 cm cavitary lesion with asymmetric thick wall in the right upper lobe, with a small amount of surrounding ground glass opacity (Figure 7). There are multiple small pulmonary nodules consistent with the patient's known metastatic disease, which have all decreased in size compared to the prior study (not shown). Ā |