General Discussion: Full Patient History:
The patient is a 26 year old male with T-cell lymphoma, status post 3 cycles of chemotherapy. He developed lower back pain, and sacroilitis was found on PET-CT #1. Subsequent biopsy and culture showed coagulase negative Staphylococcus septic arthritis. He was treated with intravenous antibiotics.
General Discussion:
Infection of the sacroiliac joint is extremely rare; fewer than 200 confirmed cases are reported in the English language literature. Its initial manifestations always mimic those of more common conditions, including low back pain, ruptured disk with sciatica, intra- or extra-pelvic abscess, psoas abscess, hip sepsis, abdominal infection, and pyelonephritis or kidney stones.
The etiology of this infection is generally accepted as the hematogenous spread of an organism to the highly vascular anterior sacroiliac region; in about half the cases, a remote, preexisting infection can be identified as the source of the responsible bacterium. Although this problem occurs among all age groups (with a possible 2:1 bias toward male patients), the majority of cases seem to occur in children and young adults. Staphylococcus aureus is the most frequently reported causative organism, but other infections have involved Streptococcus sp, Bacillus
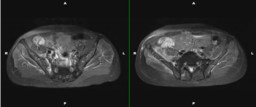
Early in the clinical course of this infection, pelvic radiographs almost always yield negative results; before the 1990s, the most reliable and recommended study for the early diagnosis of septic sacroiliitis was a bone scan. More recently, however, several reports have shown MRI of the pelvis to be far more sensitive and specific than nuclear medicine studies in rendering a correct diagnosis of sacroiliac infection
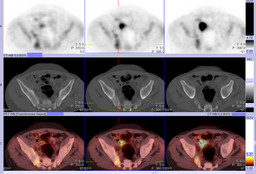
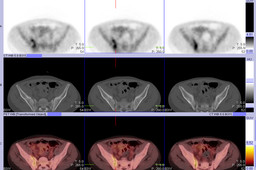
In this case, sacroiliitis was found incidentally on a PET-CT requested for monitoring treatment response of lymphoma. The linear pattern of FDG uptake in the right sacroiliac joint, without bone erosion, is suggestive of joint inflammation and/or infection. Subsequent pelvic MRI is supportive of this diagnosis. Joint aspiration and culture confirmed the diagnosis of septic sacroiliitis. Increased FDG uptake in the right sacroiliac joint seen on PET-CT #2 after weeks of intravenous antibiotic treatment likely indicates active disease.
Ā