|
| Patient: male |
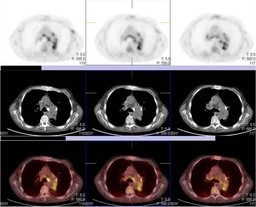
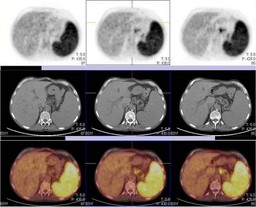
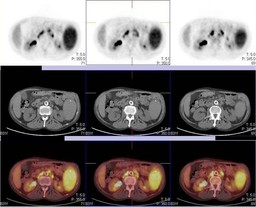
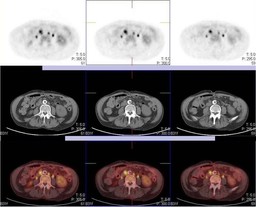
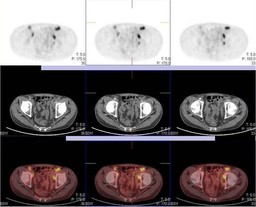
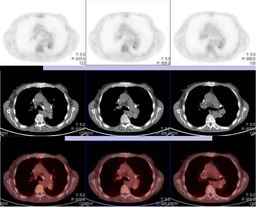
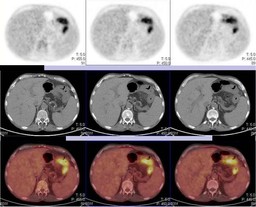
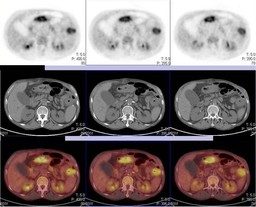
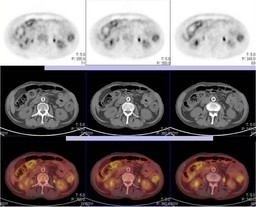
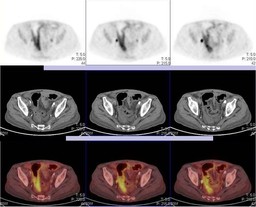
| History: 65 year old man presents for restaging after completion of therapy Ā Figure 1 Figure 2 Figure 3 Figure 4 Figure 5 Figure 6 Figure 7 Ā What is your interpretation of the study?Ā Ā The patient received an autologous stem cell transplant Ā One month after autologous stem cell transplantation Ā Figure 8 Figure 9 Figure 10 Figure 11 Figure 12 Figure 13 Figure 14 Ā What is your interpretation of the follow up study? Ā Is there an important non-oncologic finding? |
Image Size:
|
| Findings: Restaging after completion of therapyĀPET-CT Report Ā RADIOPHARMACEUTICAL: 12.4 mCi F-18 Fluorodeoxyglucose i.v. Ā 1. Interval progression of disease with increased FDG uptake in cervical, mediastinal, hilar lymph, mesenteric, retroperitoneal and inguinal lymph nodes as well as abnormally increased FDG splenic uptake, increased compared to prior exam. Ā 2. Stable left upper lobe spiculated nodule with blood pool level FDG uptake. Given the low uptake in the nodule relative to the patient's lymphadenopathy, this lesion is unlikely due to lymphoma. Continued imaging follow up is recommended as this nodule may represent a primary lung cancer such as bronchioloalveolar carcinoma. Ā One month after stem cell transplantĀPET-CT Report Ā RADIOPHARMACEUTICAL: 13.3 mCi F-18 Fluorodeoxyglucose (FDG) i.v. Ā 1. Marked interval response to therapy with minimal to mild FDG uptake in hilar and subcarinal lymph nodes likely representing residual disease. Ā 2. Interval development of diffusely increased colonic FDG uptake with wall thickening and inflammatory stranding.ĀĀ Ā 3. Interval development of multiple pulmonary nodules with minimal to mildly increased FDG uptake, likely inflammatory in etiology. Ā 4. Spiculated left upper lobe pulmonary nodule with blood pool level FDG uptake, unchanged compared to prior exam. This nodule may represent a low grade primary lung cancer, and continued follow up is recommended. |
| DDx: New diffusely increased colonic FDG uptake: Ā 1. Infectious Colitis Ā 2. Inflammatory Colitis Ā 3. Atypical pattern of lymphomatous involvement of the colon |
| Diagnosis: DiagnosisĀafterĀrestaging PET-CT: Ā Interval progression of angioblastic T-cell lymphoma (compared toĀa priorĀPET-CT, 3 months earlier) Ā Diagnosis one month after stem cell transplant: Ā Stool Specimen positive for Clostridium difficile toxin on 12/28/2009 Ā |
| References: Arango et al. "Incidence of Clostridium difficile-associated diarrhea before and after autologous peripheral blood stem cell transplantation for lyphoma and multiple myeloma" Bone Marrow Transplantation. 37, 517-521. 2006 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 238067 The reader is fully responsible for confirming the accuracy of this content. |