General Discussion: Full Patient History :
59-year-old Caucasian man with colon cancer diagnosed in October 2006. He had a partial colectomy with ileostomy in November 2006 and 12 cycles of chemotherapy. His last chemotherapy was 2 weeksĀbefore PET/CTĀwas requested. He reported chronic diarrhea and fatigue. He denied fever, wheezing, productive sputum, hemoptysis, shortness of breath or night sweats.
Discussion :
An association of sarcoidosis with malignancy has been reported and may represent a generalized reaction to the malignancy.Ā Sarcoid like reaction (SLR) has also been reported after chemotherapy for malignant tumors. Sarcoidosis and SLR in lymph nodes are mostly reported in patients with testicular cancer and lymphomas, although other tumors such as papillary thyroid carcinoma, leiomyosarcoma of the stomach, and colon cancer have also been reported in association with systemic sarcoidosis. SLR has also been reported after interferon therapy in patients with malignant melanoma and after interleukin-2 therapy for renal cell carcinoma.
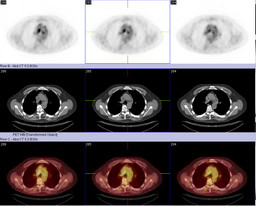
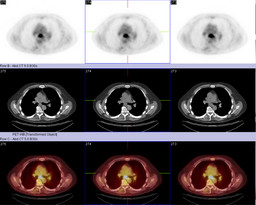
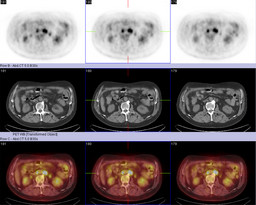
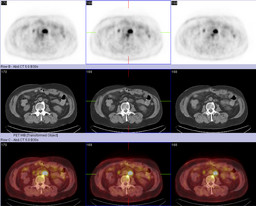
It is generally accepted that an SUVĀof 2.5 in FDG-PET scans is suggestive of malignancy. However, FDG may accumulate in areas of inflammation, such as active granulomatous foci, where lymphocytes and macrophages accumulate. Active granulomatous processes such as tuberculomas, sarcoidosis, cryptococcosis, and pneumocystis infections have been reported to be associated with increased FDG uptake. It should be remembered that FDG uptake is indicative of high metabolic activity and not necessarily of a malignancy.
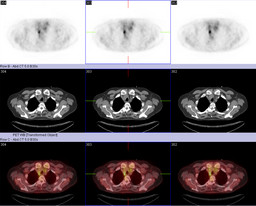
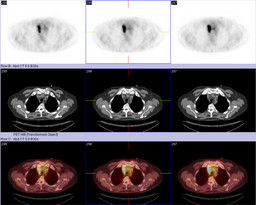
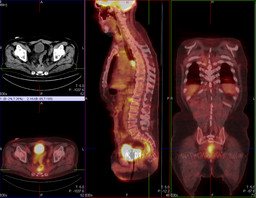
Our patient had known colon cancerĀand involvement of multiple mediastinal lymph nodes. Colon cancer most commonly metastasizes to the regional lymph nodes, liver, bone, lung, and brain. However rare, metastases to mediastinal lymph nodes from colorectal carcinomas have also been reported. The postulated mechanism is spreading via the lymphatic drainage routs of the liver in those patients with concurrent liver metastases, or via the paravertebral or paraaortic lymphatic plexus in those patients with abdominal or pelvic disease.
It is proposed that the occurrence of sarcoidosis/SLR is a reactive process to the malignant tumor. This is supported by the fact that development of sarcoidosis/SLR or worsening of preexisting disease has been observed in patients with a malignancy who may have or have not received chemotherapy. The SLR may represent a granulomatous response to a soluble antigen that is produced by the tumor and is further processed by dendritic cells. Indeed, SLRs are usually seen in lymph nodes or organs that are uninvolved by the tumor but are accessible to dendritic cells. Tumor-infiltrating dendritic cells have been reported as a favorable prognostic factor, as has SLR in some tumors. Treatment of the underlying malignancy may lead to the regression of sarcoidosis/SLR.
In conclusion, our patient had a positive PET scan finding with a high SUV in mediastinal nodes that were clinically suspicious for metastatic disease from known colon primary. However, biopsy samples were negative for metastasis and contained granulomas.