General Discussion: Follow up:
Bronchoalveolar lavage of the right upper lobe was positive for Aspergillus fungatus.
Discussion: MAI Complex:
Nontuberculous mycobacteria associated with lung disease (COPD) or immunocompromise.Clinical symptoms are like TB.No human to human spread.
Radiologic appearance in non-immunocompromised patients (usually COPD):
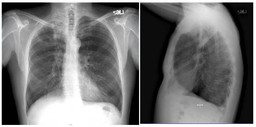
• CXR-linear and nodular opacities in apical and posterior upper lobe and superior lower lobe, bronchiectasis, fibrosis, atelectasis
• CT-centrilobular nodules (tree-in-bud), multilobe bronchiectasis (often lingula and RML), consolidation, cavitation, fibrosis, atelectasis
Radiologic appearance in immunocompromised patients can vary:
• Normal, pleural effusion, consolidation, miliary
• Pulmonary Aspergillosis: Saprophytic aspergillosis (aspergilloma,mycetoma, fungus ball)
– Usually colonizes pre-existing cavity (TB, sarcoid, neoplasm)
– Intracavitary mass, air-crescent
• Allergic bronchopulmonary aspergillosis
– Allergic reaction to antigens
– Associated with asthma and CF
– Consolidation and bronchiectasis
• Chronic necrotizing pulmonary aspergillosis (semi-invasive)
– Associated with mild immunocompromise (steroids), DM, alcohol, COPD
– Upper lobe cavitary consolidation
• Invasive pulmonary aspergillosis
– Associated with neutropenia of AIDS, malignancy, transplant
– Early nodules and air-space consolidation, late cavitary lesions, hemorrhagic necrosis (halo sign)