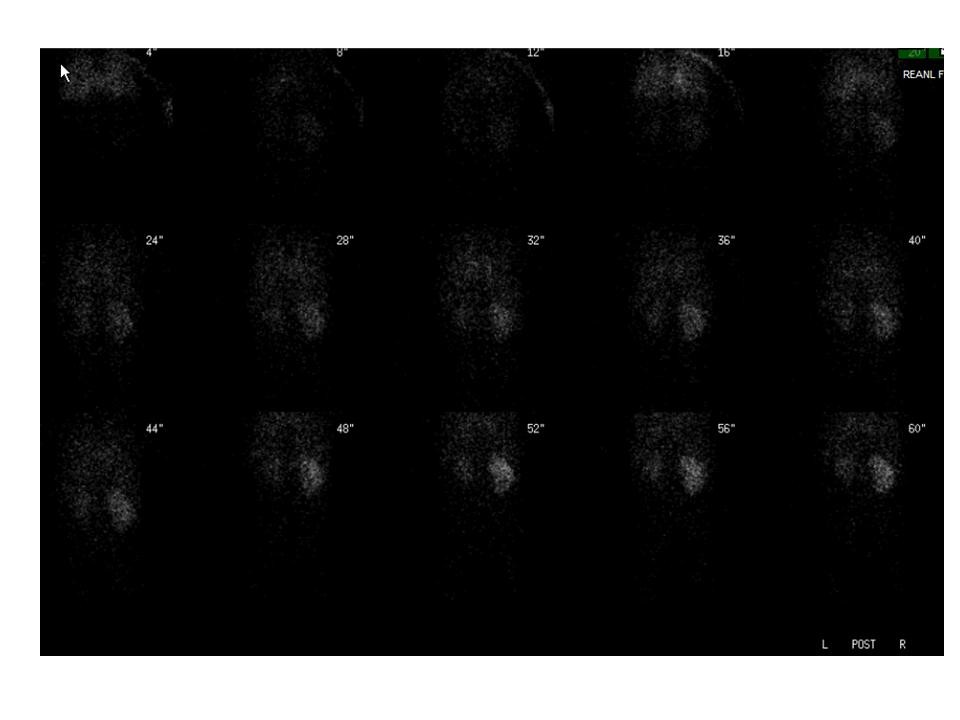
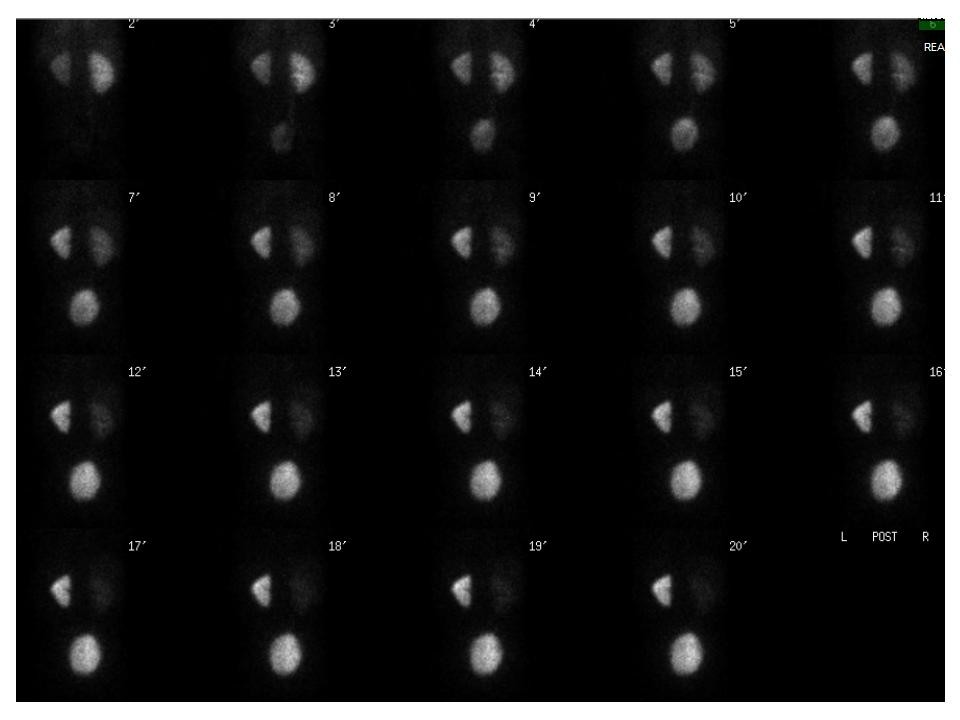
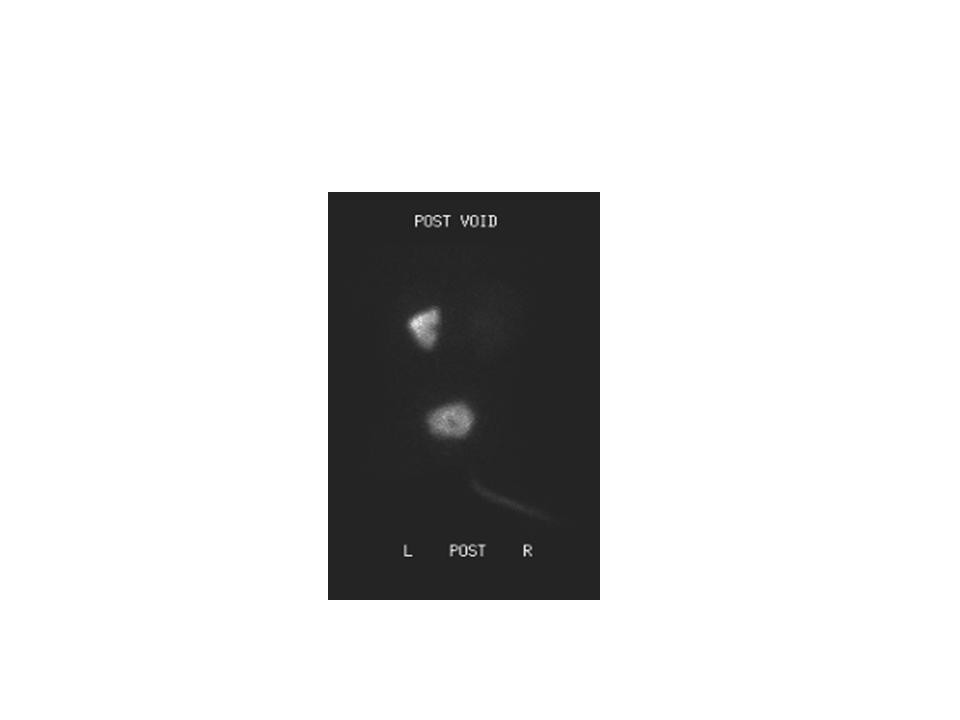
| Findings: Renal scintigraphy demonstrated decreased perfusion and function of the smaller left kidney, with progressively increasing renal parenchymal uptake of tracer, but no excretion. In light of the clinical history, the findings are most consistent with high-grade left renal artery stenosis. There is normal right renal function with no evidence of obstruction.
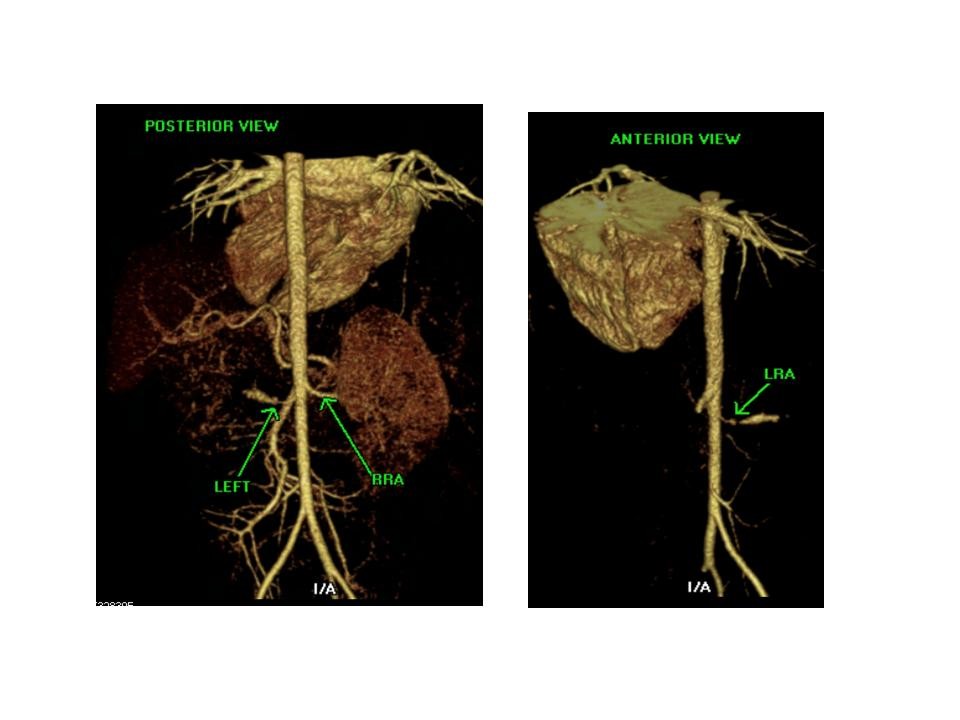
CT angiograhy deminstrated a 6 mm focal stenosis of the left renal artery in its proximal portion. Distal to the stenosis the artery caliber increases to 4 mm in diameter.
There is decreased size and a delayed nephrogram of the left kidney, consistent with focal left renal artery stenosis.
|