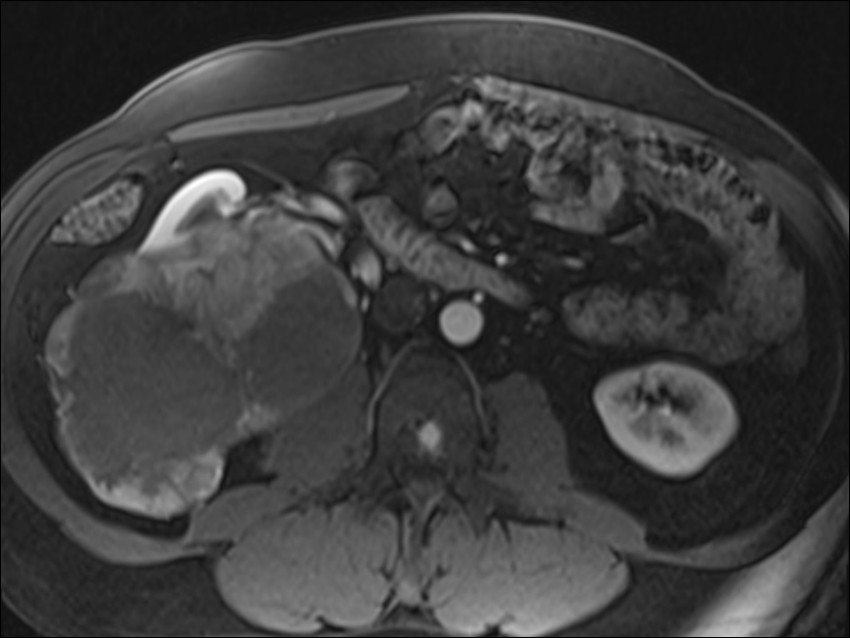
General Discussion: 57-year-old white male with recently diagnosed metastatic renal cell carcinoma with metastases to the T1,
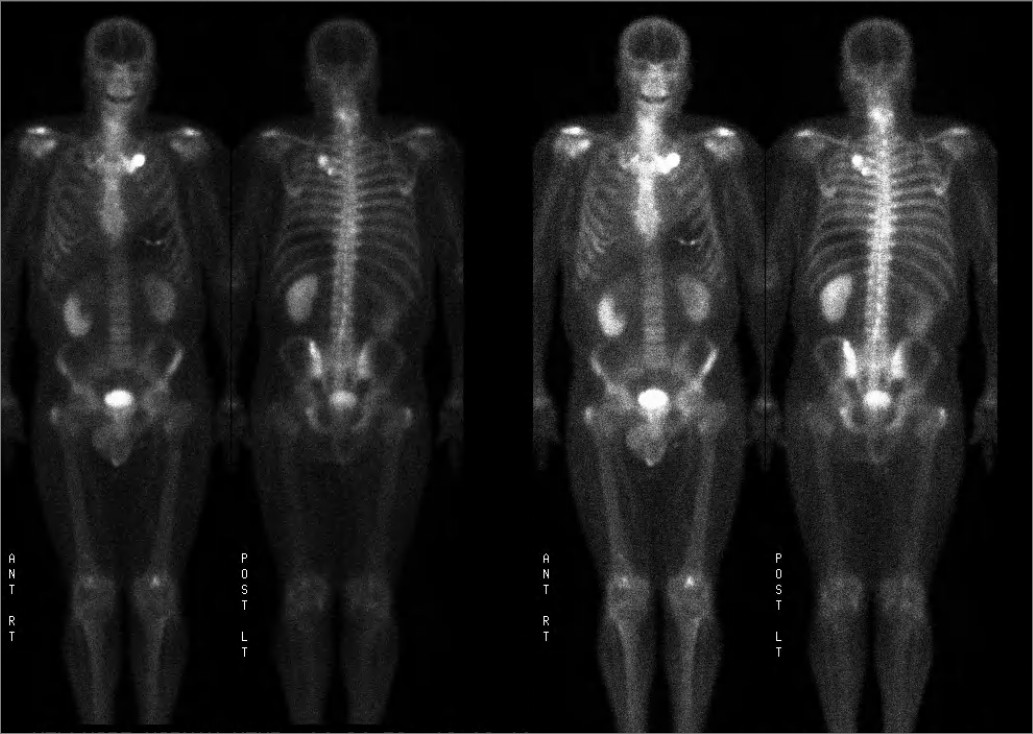
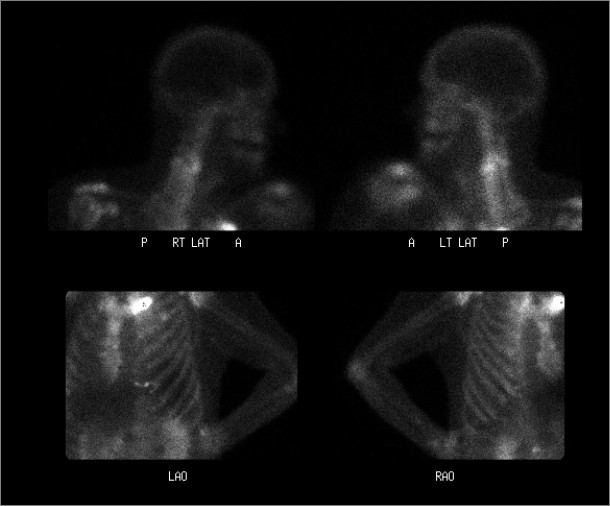
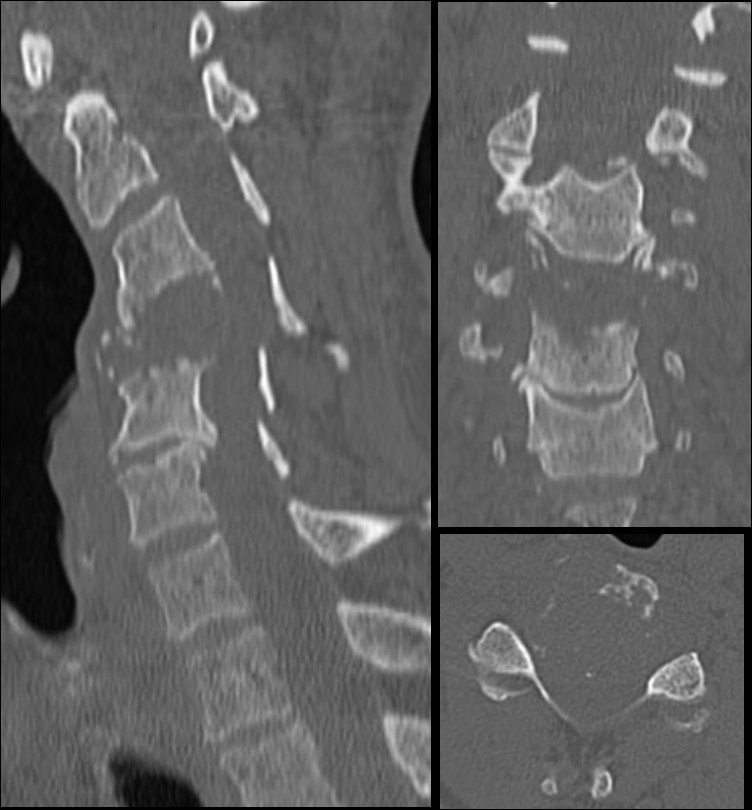
T2 and left first and third ribs and left ileum who presented to the emergency room after having several weeks of worsening neck pain. MR of the abdomen demonstrated the large renal mass with multiple metastatic lesions in the lumbar spine and in the pelvis as well as the left femoral neck. Bone scan demonstrated multiple osseous metastatic lesions in the ribs that were not known and in the pelvis that corresponded to lesion on MR imaging. Additionaly increased activity within the left aspect of mid cervical vertebral body was questioned to be degeneartive versus metastatic disease. Cervical spine radiograph and CT cervical spine showed marked destruction of the C4 vertebral body. The patient underwent surgical repair with posterior spinal fusion and excision of intraspinal extradural tumor. Additionally patient underwent chemotherapy and radiation therapy to the cervical spine.
Metastases are by far the most common malignant tumors involving the skeleton.
99m Tc methylene diphosphonate (MDP) is an effective method for screening the whole body for bone metastases.
Patients with bone metastases may present with complications such as neurologic impairment due
to spinal epidural compression which should be treated emergently. Bone scintigraphy findings are highly sensitive but nonspecific.
Metastatic disease occurs in a significant percentage of patients with renal cell carcinoma. Osseous metastases from RCC show variable uptake on bone scintigraphy. There may be focal photopenia if the lesions are purely lytic without associated reactive bone formation. It has been shown that the sensitivity of bone scintigraphy in RCC varies from 10% to 60%, even among preselected patients with a high probability of skeletal involvement.
In this case of renal cell carcinoma, bone scintigraphy was helpful in detecting cervical vertebral metastasis and additional lesions
that were previously not known. Activity in spine, particularly mid to lower cervical spine and lumbar spine can be non-specific and easily attributed to degenerative disease. In a patient with known malignancy and other metastatic osseous foci, high level of suspicion should be kept for increased activity in spine and should be correlated with other imaging modalities such as plain radiograph, CT scan or MRI.