|
| Patient: 4 year old male |
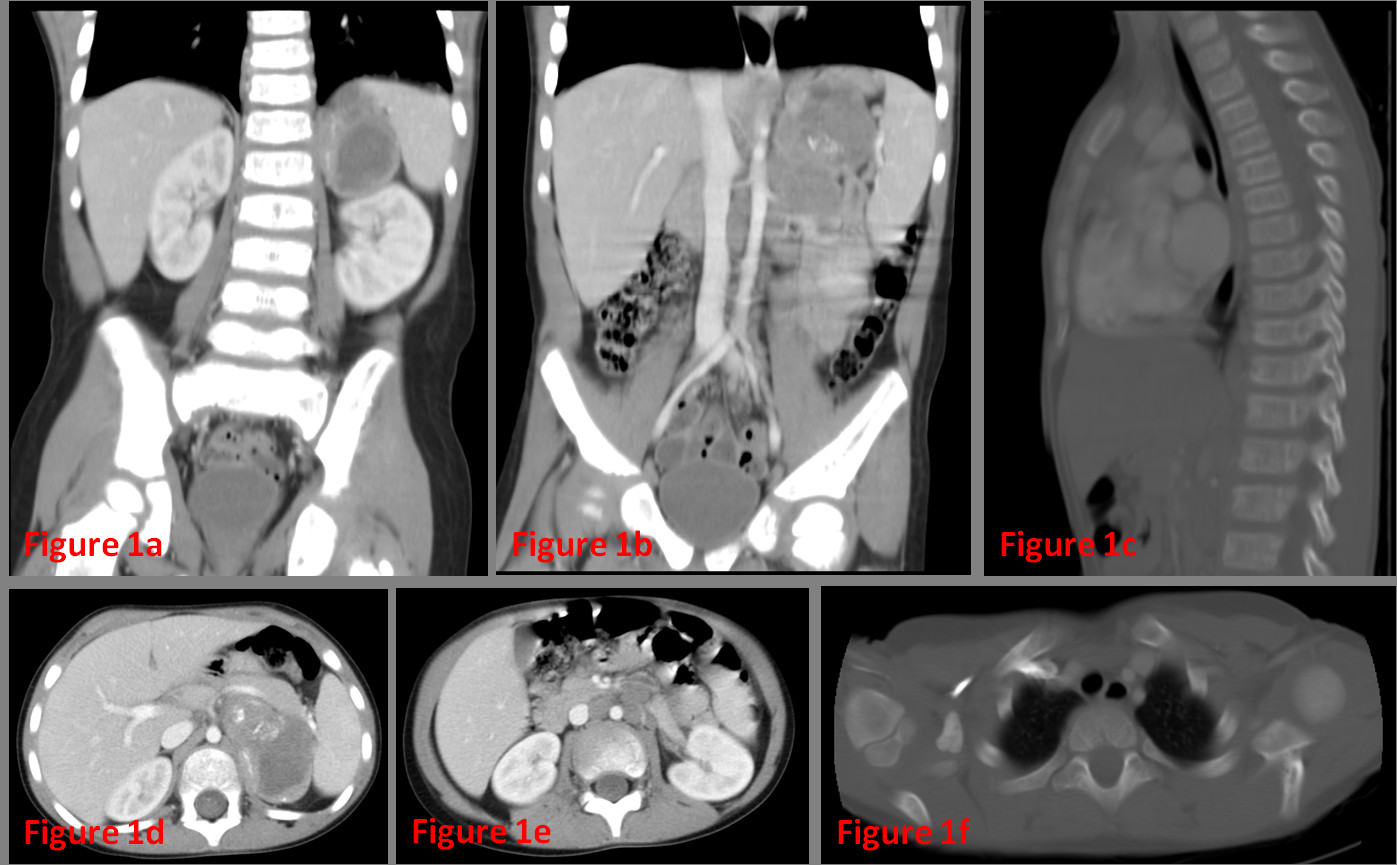
| History: 4 year old male, presented with increasing fatigue and easy bruising of lower extremities and around eyes. |
Image Size:
|
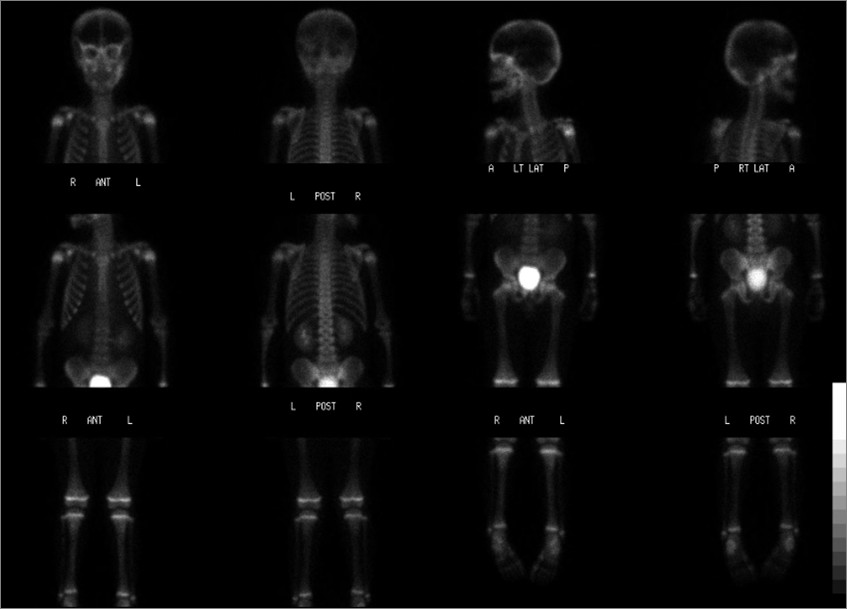
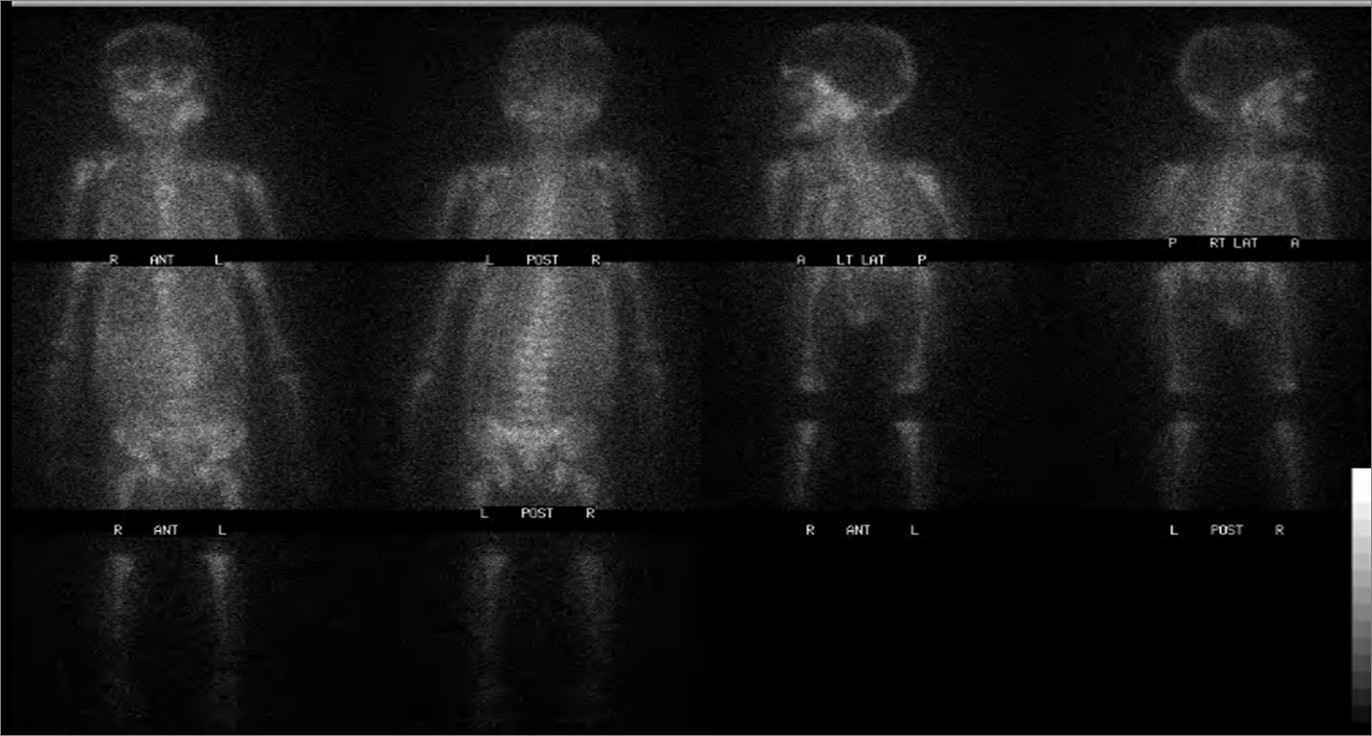
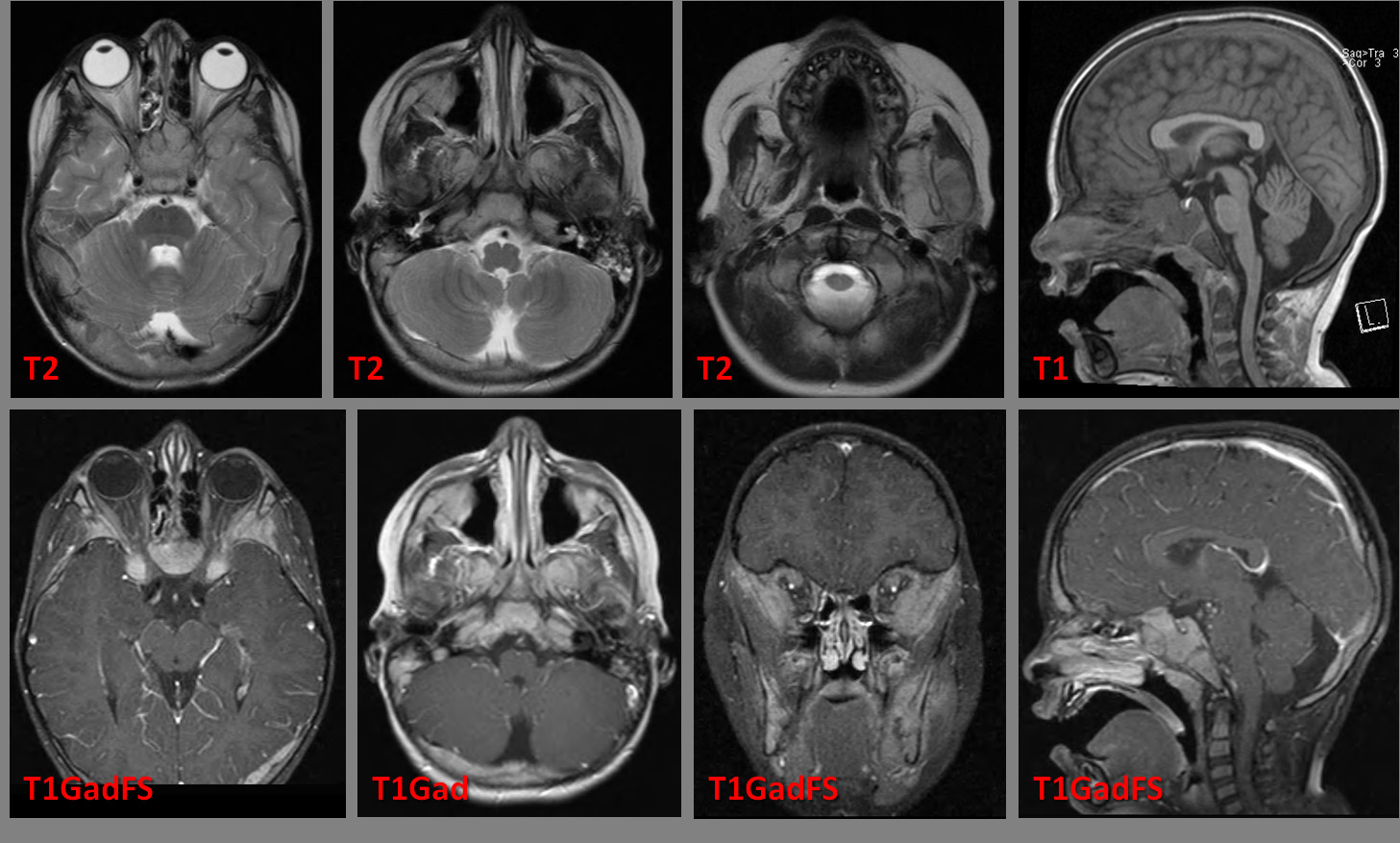
| Findings: Contrast enhanced CT images of the abdomen (Figure 1). Figure 1 findings: There is a heterogeneously enhancing, centrally necrotic, partially calcified mass arising from the left adrenal gland, associated with multiple adjacent enlarged retroperitoneal lymph nodes. Markedly enlarged aortocaval lymph node is demonstrated on the on the coronal and axial images (Figure 1b and 1e). There is diffuse osseous metastatic disease involving numerous thoracic vertebral bodies (Figure 1c), the bilateral clavicles, scapula (Figure 1f), the bones of the pelvis (not shown), as well as likely the ribs bilaterally. There is mild loss of height of numerous thoracic vertebral bodies. As part of the staging two scintigraphic images were preformed, Figure 2 and Figure 3. Identify the tracer and describe the abnormal findings. Figure 2: Radiopharmacheutical: 5.6 mCi Tc-99m MDP IV. Findings: The delayed whole-body scintigraphic images demonstrate relatively mild increased uptake in the calvaria, especially in the orbits and asymmetric increased activity in the left mandible. There is apparently normal distribution of activity throughout the rest of the skeleton. The photopenic area overlying the superior pole of the left kidney is consisted with the known adrenal mass. Figure 3: Radiopharmaceutical: 3 mCi I-123 metaiodobenzylguanidine (MIBG) IV and 3 drops SSKI solution p.o. once daily for 2 days beginning 30-60 minutes prior to tracer administration. Findings: Images of the head, neck, trunk, and proximal extremities were obtained 24 hours after administration of I-123 MIBG. Abnormal MIBG uptake is present throughout the axial and appendicular skeleton consistent with diffuse osseous metastases. In correlation to the bone scan there is increased uptake at the base of skull, orbits and left mandible. However the MIBG scan better delineates the widespread osseous metastases, since no bone or bone marrow should be visible on a normal MIBG study. Presented MRI Images of the head and orbits, Figure 4. The high contrast resolution of the T1, T2 and T1 post gadolinium demonstrate the extent of the involvement. MRI findings, Figure 4: Diffuse bone marrow replacement is seen throughout the facial bones and skull base (Sagittal T1GadFS) specifically involving the bilateral sphenoid wings (Axial T1GadFS), zygomatic arches (not shown), the mandible, the maxilla, and the clivus. The expanded sphenoid bone and clivus resulting in obliteration of the sphenoid sinuses and narrowing of the sellar turcica with compression of the pituitary gland. There is diffuse tumor involving the maxillary bone and the orbital bones with extra osseous tumor extension into the extraconal space of the orbit bilaterally (Coronal T1GadFS). Multiple ossseous lesions are identified throughout the calvaria specifically involving the right frontal bone and the right occipital bone(AxialT1Gad). The tumoral involvement of the mandibular rami extend to the adjacent masticator spaces, more prominent on the left side (Coronal T1GadFS).
|
| DDx: Differential Diagnosis: Wilm’s tumor, Ewing Sarcoma, rhabdomyosarcoma, leukemia, lymphoma might be tumors to consider in this age group. However, the MIBG study strongly favors a neuroendocrine tumor such as neuroblastoma. |
| Diagnosis: Poorly differentiated stage IV Neuroblastoma of the left adrenal gland |
| References: Radiology Review Manual, Dahnert, Fourth Edition, LWW |
| Comments: No comments posted. |
| Additional Details:
Case Number: 320157 The reader is fully responsible for confirming the accuracy of this content. |