|
| Patient: 1 month 3 day old male |
| History: One month old boy with jaundice and hyperbilirubinemia. |
Image Size:
|
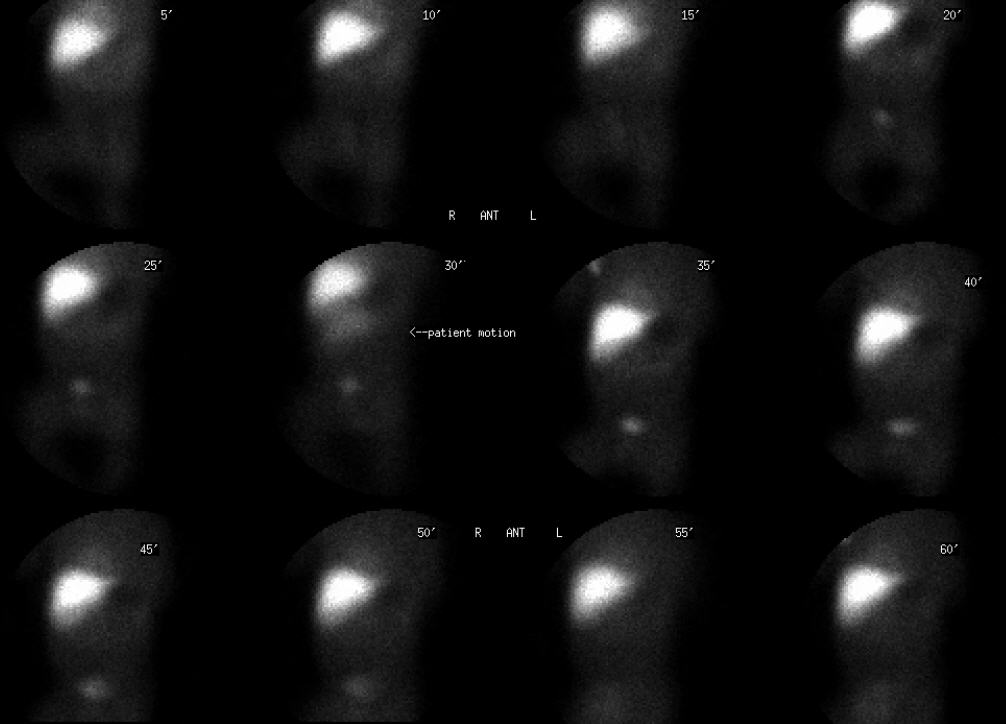
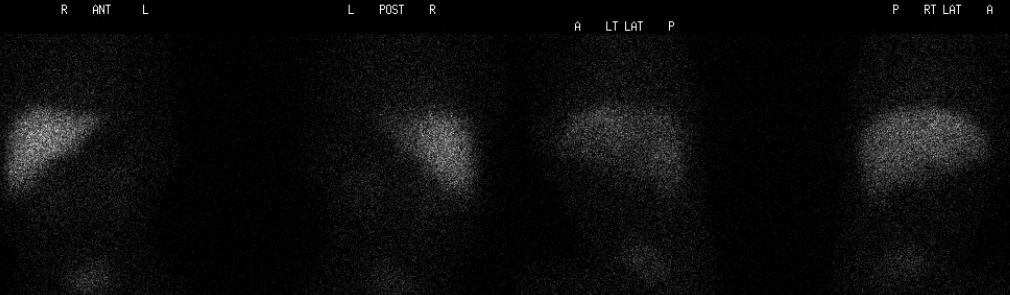
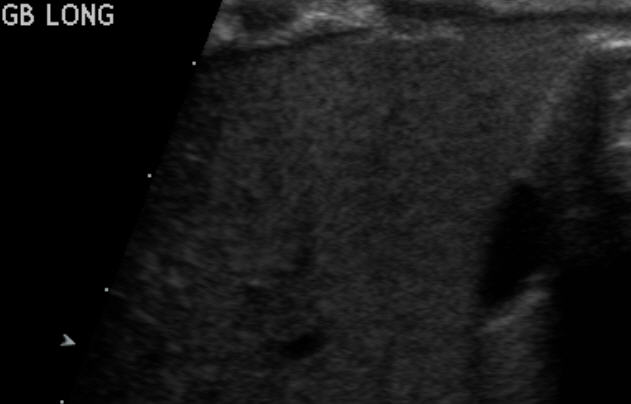
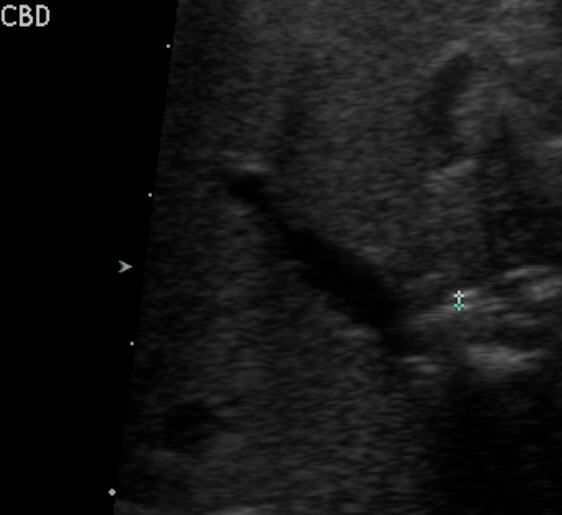
| Findings: ĀHEPATOBILIARY SCINTIGRAPHY: RADIOPHARMACEUTICAL: 0.66 mCi Tc-99m mebrofenin i.v. Ā FINDINGS: Following intravenous administration of Tc-99m mebrofenin, sequential abdominal images were obtained through 60 minutes. There is prompt, uniform accumulation of the tracer by the liver. There is no filling of the intrahepatic ducts, common bile duct or gallbladder up to 60 minutes or at 24 hours postinjection. No activity is seen within the bowel at 24 hours post injection. Ā SONOGRAPHY: There is a normal appearing liver. The gallbladder is small but normal in appearance. The common duct measures less than one mm in diameter, which is within normal limits. |
| Diagnosis: Chronic cholestasis in the setting of probable Alagille Syndrome. |
| References: http://www.emedicine.com/ped/topic60.htm - Alagille syndrome. Ann Scheimann, MD. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 313689 The reader is fully responsible for confirming the accuracy of this content. |