| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
| |||
|
|
| Patient: 15 year old |
| History: 15 year old African American male patient with Sickle cell thalassemia(hemoglobin S/beta thalassemia), presents with bilateral hip pain, worse on the right side. |
Image Size:
|
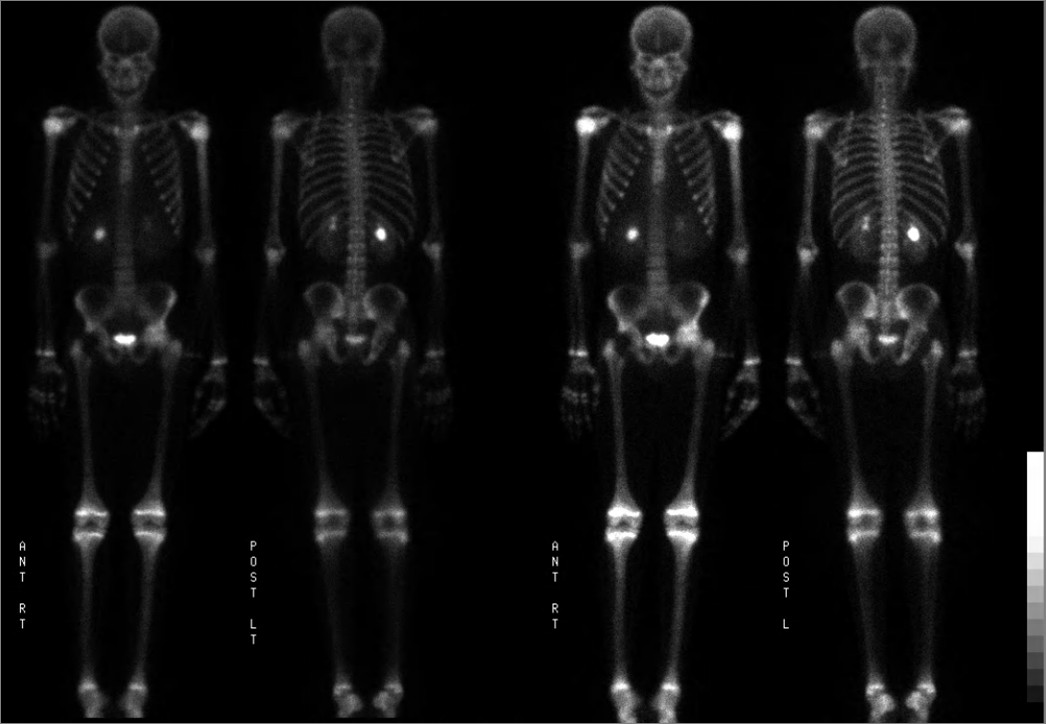
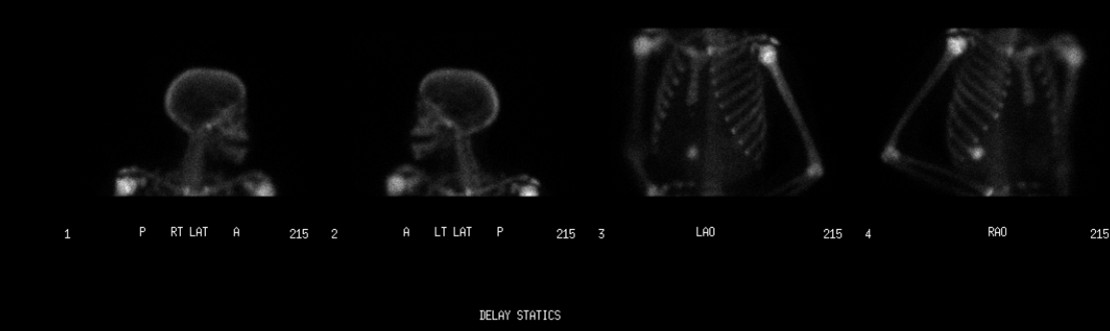
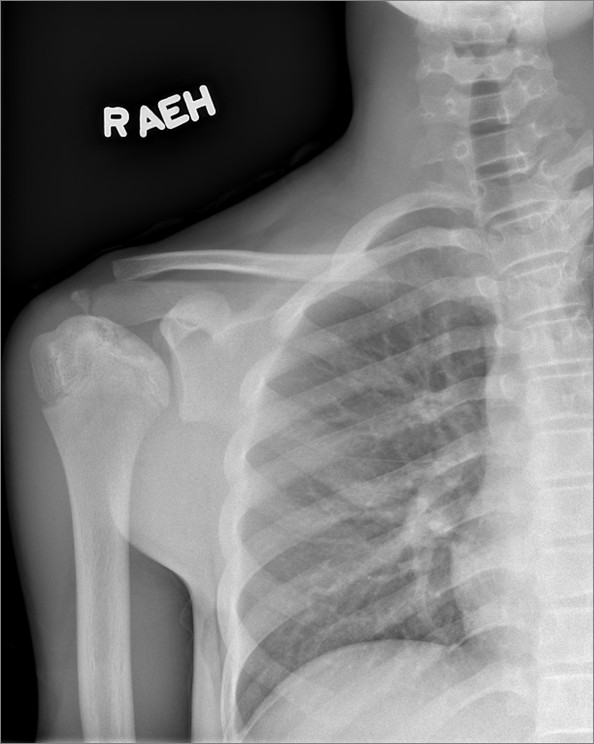
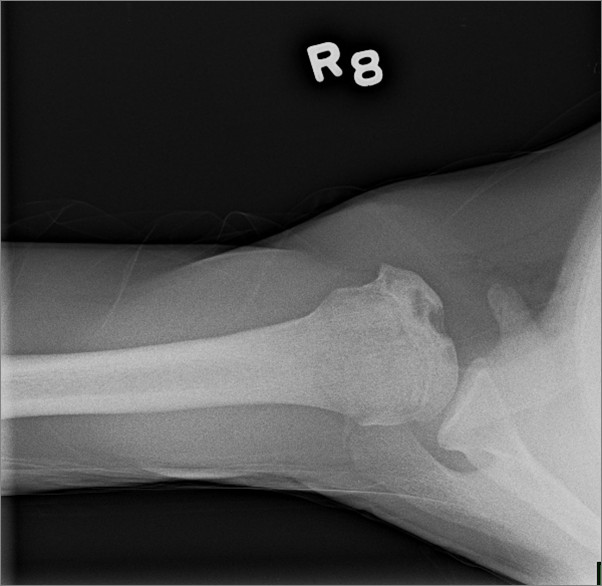
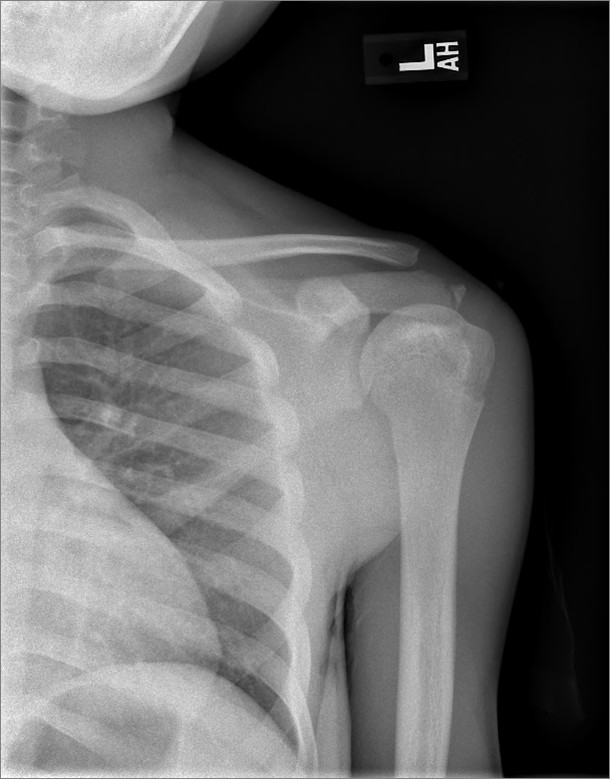
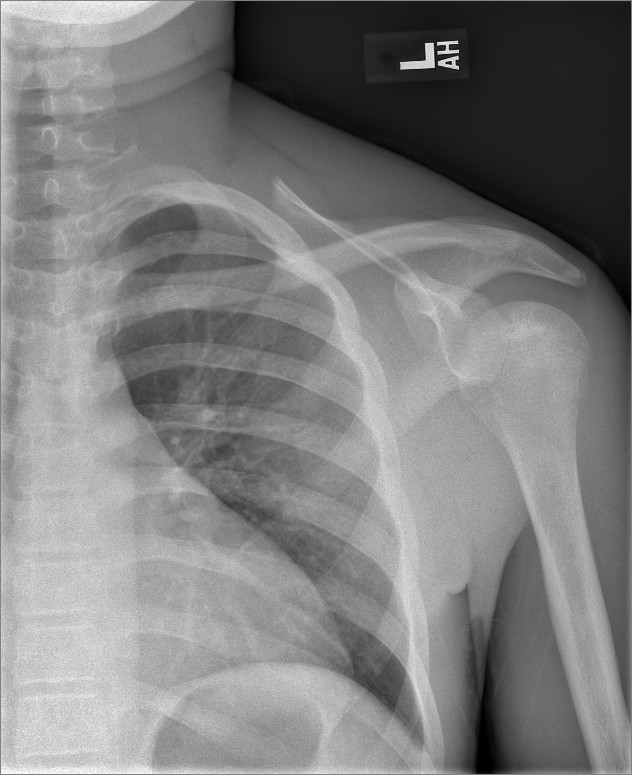
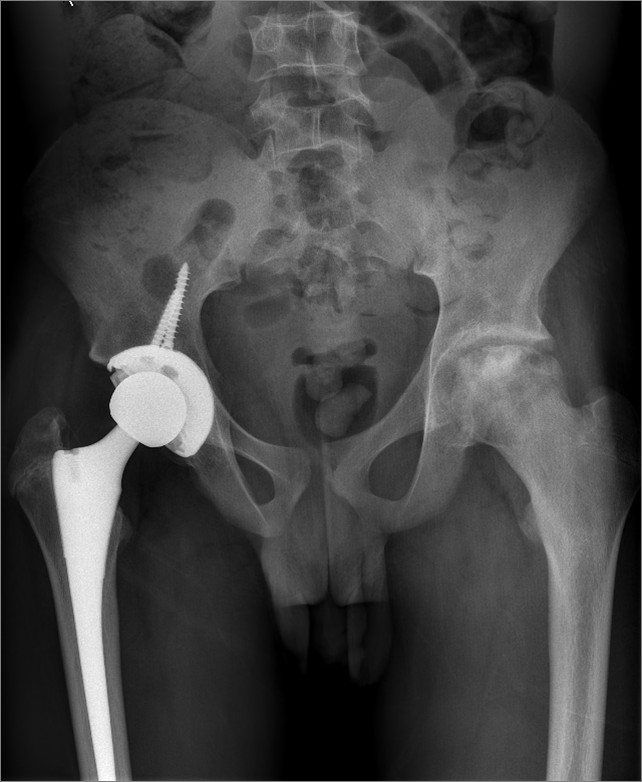
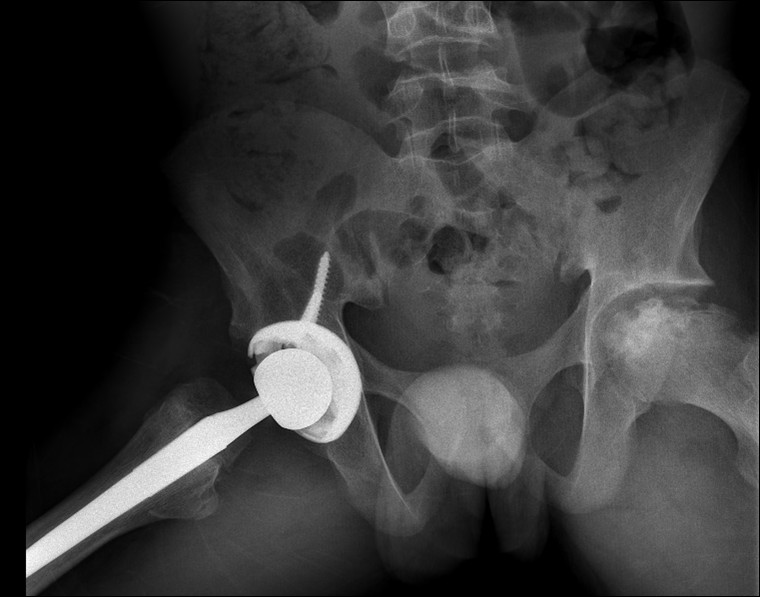
| Findings: Whole body Bone Scintigraphy done after injection of TC-99m MDP on 10/12/10 demonstrated- Diffusely increased activity in the left humerus relative to the right humerus that has no correlate in the shoulder radiographs. The diffusely increased activity in the left humerus is new since prior bone scintigraphy studies. Differential include bone infarct and infection. There is nonspecific increased activity in the left femoral head. Advanced changes of avascular necrosis of left femoral head were seen in pelvic radiograph dated 10/10/2010. The increased activity may be seen during reparative phase of avascular necrosis. Decreased activity in the right femoral head region is compatible with known right hip prosthesis seen in the pelvic radiograph.
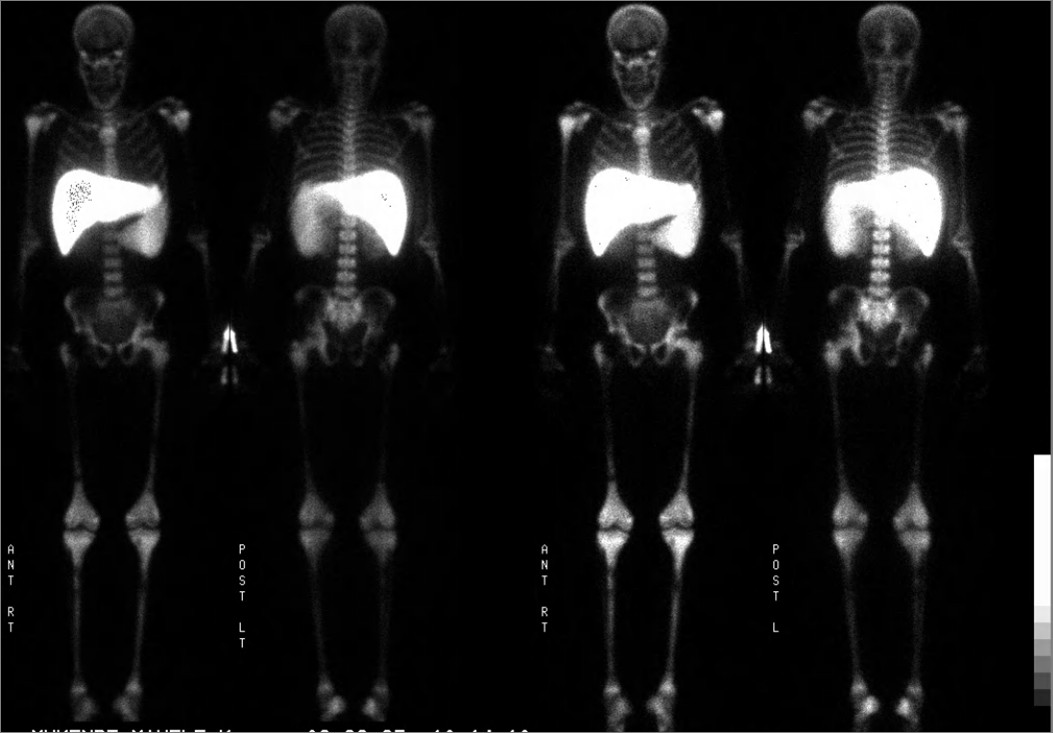
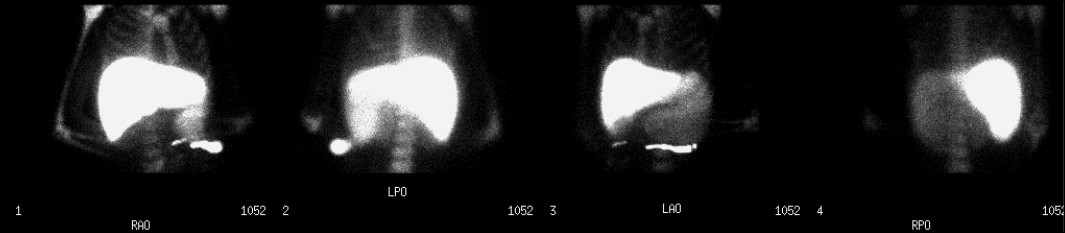
Whole Body Bone Marrow Scintigraphy done after injection of TC-99m Sulfur Colloid on10/14/10 demostrated- There is diffusely diseased radiotracer uptake in the bone marrow of left humeral diaphysis. Bone scan done on 10/12/2010 demonstrated diffusely increased activity in the left humerus. The findings from these two scans are consistent with bone marrow infarction in the left humerus. There are additional multiple foci of decreased marrow activity in the diaphysis of the bilateral femurs, tibias, and spine consistent with marrow infarction. There is also decreased marrow activity of the right ischium, and diffuse reduced activity of the right femoral diaphysis which likely represent marrow infarction and clinically correlates to the patient's increasing right hip pain. In addition, splenomegaly and expanded marrow in appendicular skeleton was visualized compatible with patient's diagnosis of sickle cell disease.
Plain Radiograph Findings: 1. Osteonecrosis of the right humeral head with a lytic component extending to the articular surface. 2. Osteonecrosis of the left humeral head without extension to the articular surface. 3. Stable right total hip arthroplasty. 4. Advanced changes of avascular necrosis in the left-side with femoral head collapse, stable. 5.Endplate changes of sickle cell disease. |
| DDx: 1. Bone Infarcts. 2. Multifocal abscesses. 3.Diffuse Metastatic disease. 4.Generalised Metabolic disorder. |
| Diagnosis: Bone Infartcs. |
| References: 1. LETTER: AN UNUSUAL BONE INFARCT IN A YOUNG ADULT SICKLER, Annals of African Medicine Vol. 4, No. 2; 2005: 91 – 93. 2.The Requisites : Pediatric Radiology 3rd Edition,Pg 176. Johan G. Blickman,Bruce R. Parker,Patrick D. Barnes. 3.eMedicine Specialities>Radiology>Musculoskeletal,Bone Infarct:Imaging, Author: Ali Nawaz Khan, MBBS, FRCS, FRCP, FRCR, Coauthor(s): Mohammed Jassim Al-Salman, MBBS, Muthusamy Chandramohan, MBBS, DMRD, FRCR,Ian Turnbull, MB, ChB, MD, DMRD, FRCR, Sumaira MacDonald, MBChB, PhD, MRCP, FRCR; Charles Edward Hutchinson, MD, FRCR. 4. Scientific Article, Differentiation Between Bone Infarction and Acute Osteomyelitis in Children with Sickle-Cell Disease with Use of Sequential Radionuclide Bone-Marrow and Bone Scans , The Journal of Bone and Joint Surgery (American) 83:1810-1813 (2001),David L. Skaggs, MD, Sam K. Kim, BS, Nathan W. Greene, MD, Deborah Harris, RN and John H. Miller, MD |
| Comments: No comments posted. |
| Additional Details:
Case Number: 288897 The reader is fully responsible for confirming the accuracy of this content. |