|
| Patient: 55 year old male |
| History: Known malignancy (specific history withheld). |
Image Size:
|
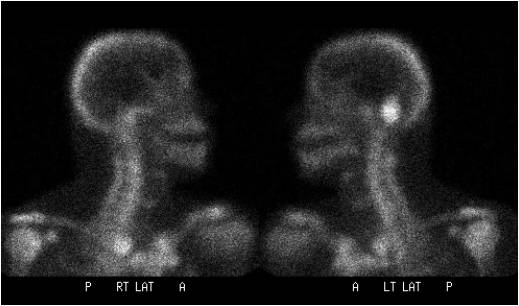
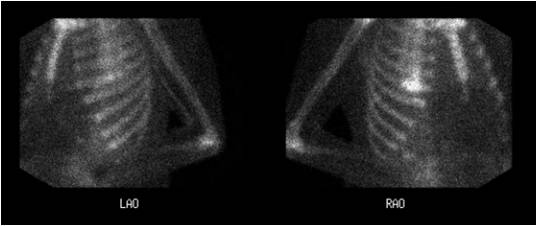
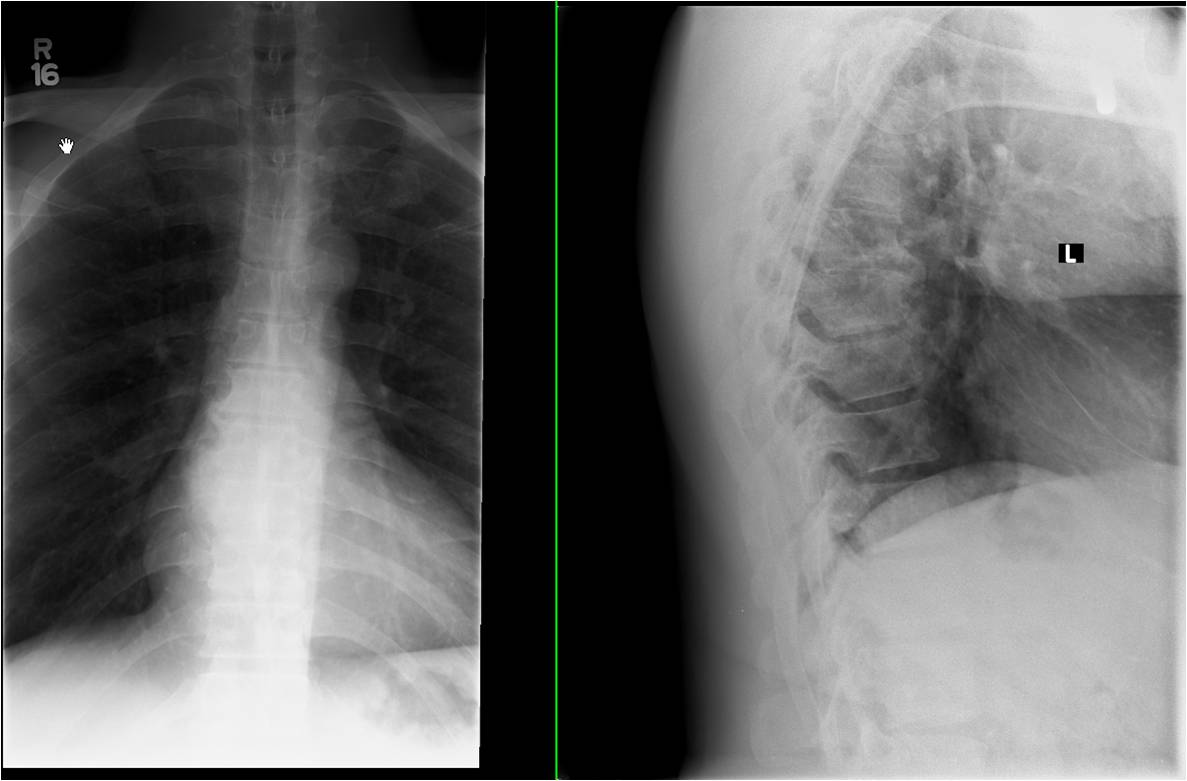
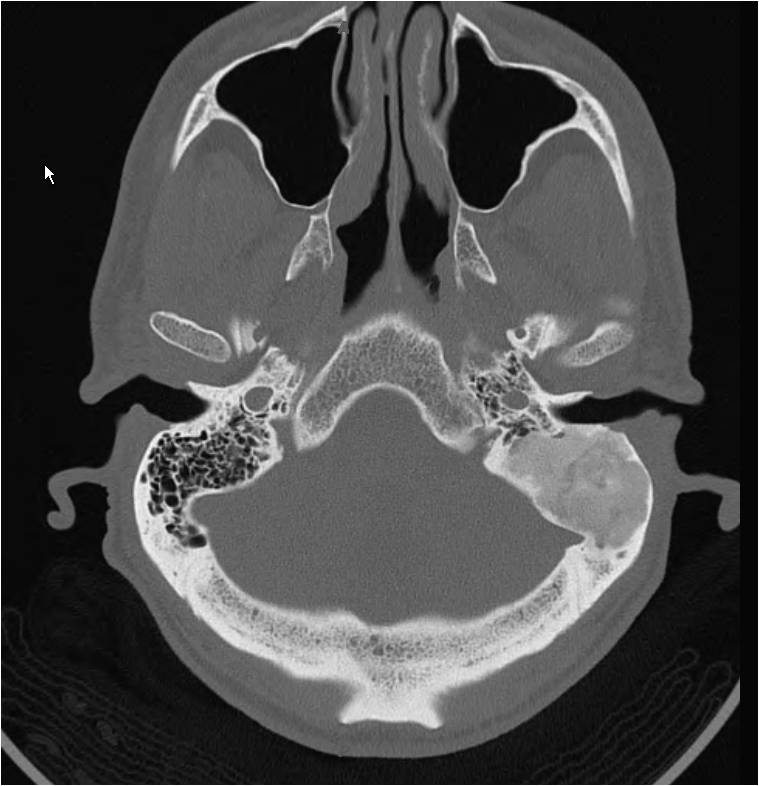
| Findings: Radiopharmaceutical: 20.8 mCi Tc-99m MDP i.v. A whole-body bone scan (Fig. 1) was performed, with additional images of the skull (Fig. 2) and ribs (Fig. 3). What are the findings? [pagebreak] These images demonstrate focal increased uptake in the region of the left mastoid air cells. There is moderate diffuse soft tissue uptake in the right anterior proximal thigh, and focal uptake in the mid thoracic spine. What additional imaging would you obtain? [pagebreak] AP and lateral thoracic spine (Fig. 4) radiographs demonstrate degenerative osteophyte formation at the T8-9 level, corresponding to the region of activity on the bone scan. Temporal bone CT (Fig. 5) demonstrates an expansile lesion of the left petrous temporal bone with ground glass matrix. |
| DDx: For the left mastoid uptake: Neoplastic (metastasis versus primary lesion) versus infectious/inflammatory process of the mastoid portion of the left petrous temporal bone vs a benign process such as fibrous dysplasia. |
| Diagnosis: Fibrous dysplasia of the mastoid portion of the left petrous temporal bone. |
| References: Brown EW, Megerian CA, McKenna MJ, Weber A. Fibrous dysplasia of the temporal bone. AJR 1995;164:679-682. Kransdorf MJ, Moser RP Jr, Gilkey FW. Fibrous dysplasia. RadioGraphics 1990;10:519-537. Nakahara T, Fujii H, Hashimoto J, Kubo A. Use of bone SPECT in the evaluation of fibrous dysplasia of the skull.ĀClin Nucl Med. 2004;29(9):554-559. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 130389 The reader is fully responsible for confirming the accuracy of this content. |