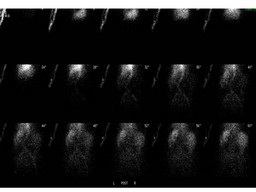
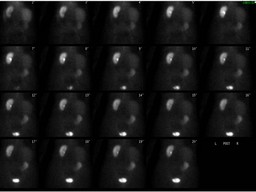
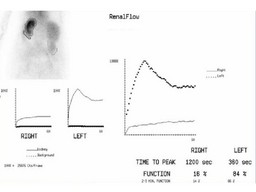
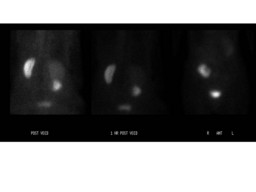
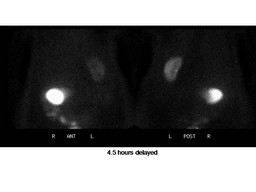
| Findings: Renal Scan: 1. Ptotic right kidney with high-grade right ureteral obstruction, as indicated by markedly delayed excretion and delayed filling of the dilated collecting system and ureter. The relative right renal function is decreased.See general discussion. 2. The parenchymal tracer retention seen on the left raises the question of superimposed medical renal disease and/or prerenal azotemia, as contributing to this patient's new renal insufficiency.
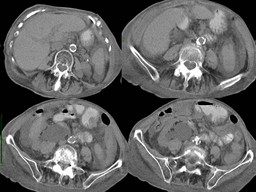
CT findings: Interval development of severe right sided hydronephrosis that appears to terminate at the ureteropelvic junction. This may be due to a metastatic deposit although none is obvious.ĀThere is a moderate-sized right-sided pleural effusion and a small left-sided pleural effusion, with a left-sided Pleurex catheter in place.
|