|
| Patient: 8 year old female |
| History: 8-year-old girl with pain. |
Image Size:
|
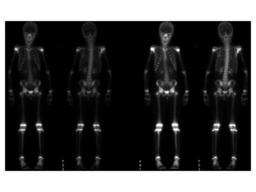
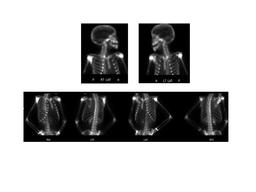
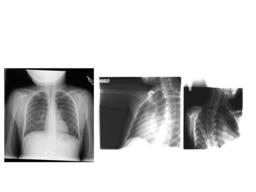
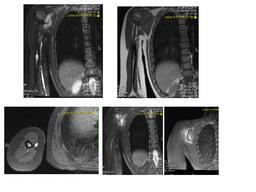
| Findings: Bone Scan: Delayed whole-body scintigrams were obtained. MRI: Large exophytic bony lesion emanating from the body of the right scapula, with large soft tissue component, concerning for Ewing sarcoma. An enhancing lesion is seen in the mid shaft of the right humerus. |
| DDx: Primary tumor - Ewing’s sarcoma - Osteosarcoma - Chondrosarcoma
Langerhans cell histiocytosis
Infection
Fracture |
| Diagnosis: LANGERHANS' CELL HISTIOCYTOSIS |
| References: emedicine:Langerhans cell histiocytosis (LCH) |
| Comments: No comments posted. |
| Additional Details:
Case Number: 91792 The reader is fully responsible for confirming the accuracy of this content. |