Specific Discussion: DISCUSSION:
WHO classification of Neuroepithelial tumors of the CNS*
1. Astrocytic tumors
2. Oligodendroglial tumors
3. Ependymal cell tumors
4. Mixed gliomas
5. Neuroepithelial tumors of uncertain origin
6. Tumors of the choroid plexus
7. Neuronal and mixed neuronal-glial tumors
Āa. Gangliocytoma
Āb. Dysplastic gangliocytoma of cerebellum (Lhermitte-Duclos)
Āc. GANGLIOGLIOMA
Ād. Anaplastic (malignant) ganglioglioma
Āe. Desmoplastic infantile ganglioglioma
Āf. Desmoplastic infantile astrocytoma
Āg. Central neurocytoma
Āh. Dysembryoplastic neuroepithelial tumor
Āi. Olfactory neuroblastoma (esthesioneuroblastoma)
Āj. Variant: olfactory neuroepithelioma
8. Pineal Parenchyma Tumors
9. Tumors with neuroblastic or glioblastic elements (embryonal tumors)
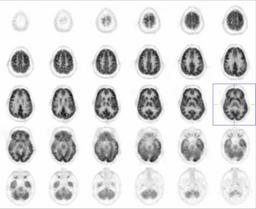
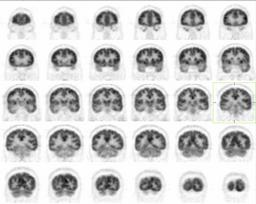
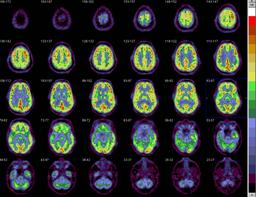
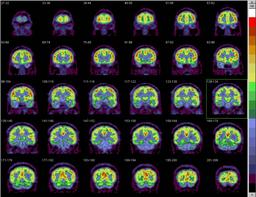
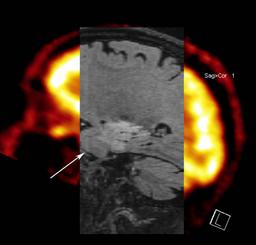
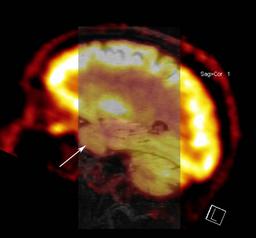
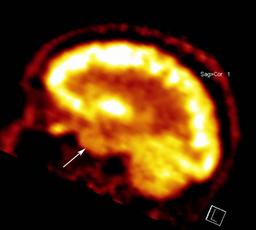
UTILIZATION OF FDG-PET IN TUMOR IMAGING:
FDG-PET in relation to tumor imaging is routinely used for the following pruposes.
1. Differentiating tumor recurrence from post-radiation necrosis
2. Predicting high- vs. low-grade primary brain tumor by evaluating the metobolic activity.
3. Prognostic indicator, by following metabolic activity after treatment.Ā