|
| Patient: 1 month 2 day old male |
| History: 4-week-old boy with urinary tract infection, and recently diagnosed right-sided hydronephrosis. |
Image Size:
|
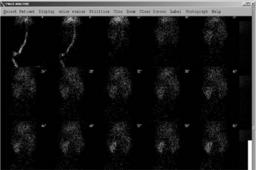
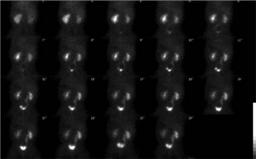
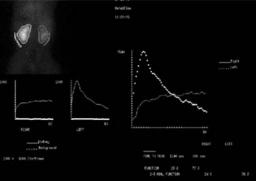
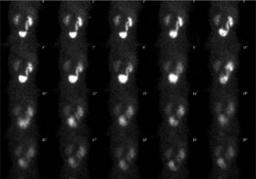
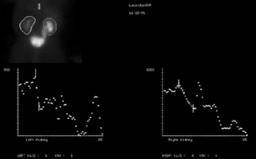
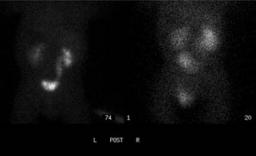
| Findings: Normal appearance and function of the left kidney.Ā Decreased right renal function, as is apparent on the images and the split function curves. No evidence for obstruction involving the right kidney based on prompt initial post-diuretic clearance of tracer.Ā However, note the strange shape of the renal curves, with bothĀfalling and risingĀof the curves. There is a dilated right collecting system and ureter with subsequently observed abrupt increase in activity in the right collecting system, easily cine on the cineĀimages, and also evident on the static display andĀtime-activity curves.ĀĀ |
| DDx: Note that patient motion (also present in this case) can cause rising and falling of the renal curves,Āsince patient motion can move the kidney in and out of the drawn region of interest. In this case, inspection of the cine and static images confirms reflux on the right. However, rising/falling on the left renal curve appears to be due to patient motion, since motion is present and no left reflux is evident on the cine images. |
| Diagnosis: Right-sided reflux during the examination. The chronic reflux likely resulted in the mildly diminished right-sided function. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 85240 The reader is fully responsible for confirming the accuracy of this content. |