| Findings: Ventilation-perfusion scintigraphy: The Tc-99m DTPA aerosol images show absence of ventilation to the entire left lung, except for a small region centrally. There is hyperdeposition of the aerosol in the intubated trachea and in the left main bronchus. The perfusion images show a physiologic distribution of pulmonary perfusion. Specifically, perfusion is well maintained to the non-ventilated left lung.
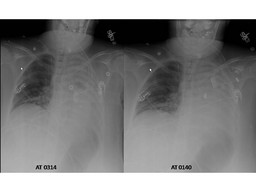
The chest radiographаinitially showed significant left sided atelectasis. After the patient was intubated, a repeat radiograph showed good position of the endotracheal tube and persistence of the left-sided volume loss. The patient had not improved and the lung scintigraphy was ordered.
Reverse ventilation-perfusion mismatching (absent perfusion with maintained perfusion) in the entire left lung. The findings indicate substantial functional right-to-left shunting and likely explain the patient's hypoxia.
аааа
|