General Discussion: Ā
ĀThe term congenital (primary) megaureter includes causes of an enlarged ureter which are intrinsic to the ureter, rather than as a result of a more distal abnormality. A ureter larger than 5 mm in diameter should be considered abnormal in childhood.Ā The megaureters can be obstructing, refluxing or refluxing/nonobstructing.
ĀThe obstructive megaureter is related to a distal adynamic segment with proximal dilatation, and is a common cause of obstructive uropathy in children. It is analogous to esophageal achalasia or colonic Hirschsprung disease although lack of ganglion cells within the wall of the ureter has not been proven to be the cause.
Refluxing primary megaureter is a result of an abnormal vesico-ureteric junction, which impedes the normal anti-reflux mechanisms. This can be due to a short vertical intramural segment, congenital paraureteric diverticulum, ureterocoele with or without associated duplicated collecting system
Non-refluxing unobstructed primary megaureter is thought to be the most common cause of primary megaureter in neonates, and even though the vesicoureteric junction is normal, with no evidence of reflux or obstruction, the ureter is enlarged. The cause for this is unknown.
Bilateral involvement is present in about 20% of patients with primary obstructed megaureters. Primary obstructed megaureter has a male-to-female ratio of nearly 4:1. The left side is more often affected than the right.
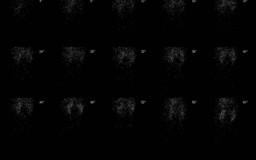
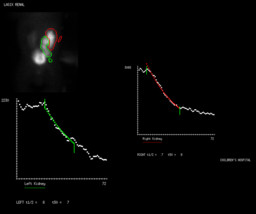
Technetium-99m mercaptoacetyltriglycine (MAG3) is the most widely employed radiopharmaceutical due to the low neonatal GFR. The diuretic renal scintigraphyĀis a useful test in determining whether a dilated collection system is functionally obstructed. The evaluation of different parameters, including differential renal uptake and time to half peak after furosemide washout, allows a reliable assessment of obstruction to the urinary flow.
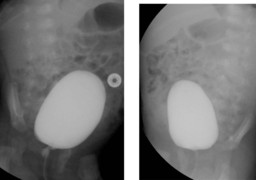
Imaging studies such as ultrasound, voiding cystourethrography and renal scan can help to differentiate primary megaureter from other causes of hydronephrosis, including ureteropelvic junction obstruction, posterior urethral valves, and ureterocele.
The treatment for asymptomatic patients with non-refluxing unobstructed primary megaureter and normal renal scan, as in the present case is nonoperative management because, in most cases, hydrouteronephrosis resolves spontaneously
Ā