|
| Patient: 47 year old male |
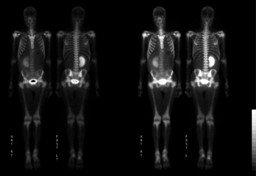
| History: 47 year-old man with cholangiocarcinoma and progressive generalized weakness admitted with altered mental status. The patient's left kidney was surgically resected (no additional information available). The following study was requested to evaluate metastatic disease. Describe the findings. What additional clinical information will be relevant for the interpretation of this study. Presented whole body bone scintigraphy study (Figure 1 and Figure 2). |
Image Size:
|
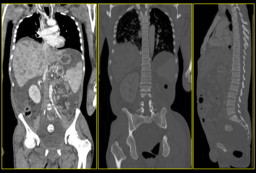
| Findings: 22.1 mCi Tc-99m MDP was administered i.v. The images demonstrate marked increased tracer uptake throughout the axial and appendicular skeleton with pronounced symetric uptake in the periarticular regions of the elbows, wrists, knees and ankles. There is no obvious evidence of osseous metastatic lesions. The hazy activity in the abdomen is related to ascites (Figure 3). There is compensatory hypertrophy of the remaining right kidney. Delineate your differential diagnosis. |
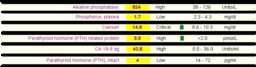
| DDx: Diffuse tracer uptake in the axial and appendicular skeleton can be seen with diffuse metastases (if little or no activity is seen in the soft tissues or urinary tract often referred as a "super scan") and in metabolic bone disease. The uptake in metabolic bone disease, such as hyperthyroidism, is more uniform in appearance and extends into the distal appendicular skeleton. Intense calvarial uptake that is disproportionate to that in the remainder of the skeleton is another feature of a metabolic etiology (not prominent in our case). Additional clinical information is provided (Figure 4) to narrow the differential diagnosis: Calcium level 14.9 mg/dL (normal range 8.6-10.3), Phosphorus 1.7 mg/dL (2.3-4.3 mg/dL), PTH 4 pg/mL (normal range 14-72), PTH related protein 5.5 pmol/L (normal <2.0), ALKP 524 Units/L (38-126). The laboratory results demonstrate moderate hypercalcemia with suppressed TSH. The differential diagnosis includes hypercalcemia associated with cancer, hyperthyroidism, adrenal insufficiency and acromegaly (if malignancy work-up is negative). Hypercalcemia associated with cancer also known as malignant hypercalcemia or humoral hypercalcemia of malignancy, is associated with elevated alkaline phosphatase and elevated PTH related protein as in our case. |
| Diagnosis: PTHrP Malignancy-Associated Hypercalcemia |
| References: Basso U. et al; Malignant Hypercalcemia, Current Medicinal Chemistry 2011;18:3462-3467 A.F. Stewart; Hypercalcemia Associated with Cancer, NEJM 2005;352:373-9 C. Love et al; Radionuclide Bone Imaging: An Illustrative Review, RadioGraphics 2003;23:341-358 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 385072 The reader is fully responsible for confirming the accuracy of this content. |