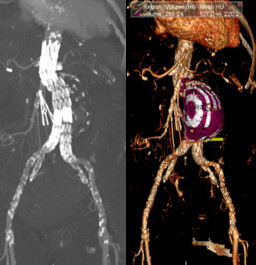
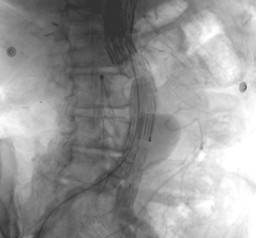
General Discussion: This was a 79-year-old female patient on hemodialysis with known abdominal aneurysm, status post endovascular repair 3 months prior. Patient now presents with unexplained anemia not responding adequately to transfusions. The patient had CT abdominal angiography that demonstrated a large endoleak located near the proximal aspect of the iliac limbs, likely a type II endoleak. Abdominal aortic angiography later demonstrated Type I B endoleak from the distal landing zone of the right iliac stent
graft and a Type II endoleak along the left iliac stent graft filling from a small left lumbar artery. As patient completed the angiography, she had a large bloody bowel movement and there was concern for aorto-enteric fistula. The GI bleed study was positive for an upper GI bleed likely from the duodenal bulb and was not adjacent to the aneurysmal sac. Patient subsequently underwent upper GI endoscopy demonstrated one gastric ulcer and 2 duodenal ulcers with adherent clot. These ulcers were injected, heater probed, and clipped. The 3rd part of the duodenum and 4th part of the duodenum were normal
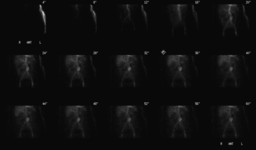
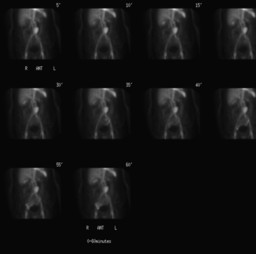
Gastrointestinal bleeding scintigraphy is done in patients suspected of active gastrointestinal bleeding using Tc-99m labeled red blood cells (RBCs). The sites of active bleeding are identified by the accumulation and movement of labeled red blood cells within the bowel lumen. The activity within the lumen of the bowel can move antegrade as well as retrograde. Cine display of the images increases the accurate localization of the site of bleeding.
Common causes of upper GI bleeding include esophageal varices, gastric and duodenal ulcers, gastritis, esophagitis, Mallory-Weiss tears or neoplasms.
Endoscopy and angiography provide accurate localization and potential therapeutic control of bleeding sites. Scintigraphy
permits continuous monitoring over hours which is a major advantage over intermittent sampling since most bleeds are intermittent and may be missed by endoscopy or angigraphy.
Aorto-enteric fistula (AEF) is a rare cause of GI bleed and when present is associate with high mortality. High level of suspicion is hence desirable in patients with known aortic aneurysm espcially those with prior intervention for aneurysm repair. The most common site of AEF is the third part of duodenum. An aortoenteric fistula results from the erosion of the aortic graft into the bowel lumen, usually the third or fourth portion of the duodenum. The result is a direct communication between the aortic graft lumen and the bowel lumen.