|
| Patient: 50 year old male |
| History: 50 year old male with recent diagnosis of left distal ulnar mass, presumed to be a malignant lesion. Evaluate for bony metastasis. |
Image Size:
|
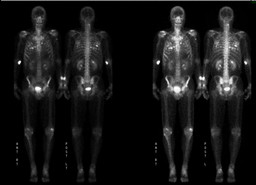
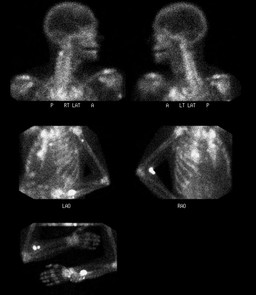
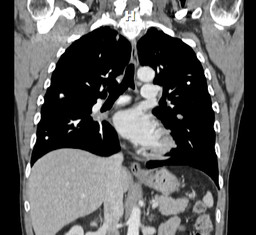
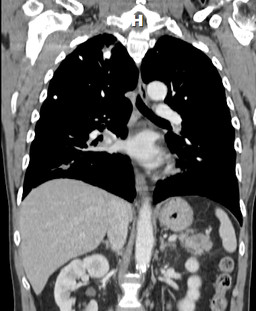
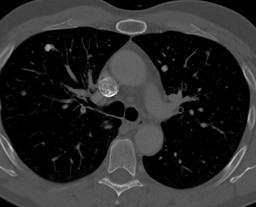
| Findings: Bone Scintigraphy: There is increased focal uptake in the left distal ulna, just proximal to the expanded distal expansile lesion. Focal uptake is also identified in the left proximal humerus. Focal increased activity in the region C2 vertebral body on the left side, could be in the pedicle. Numerous foci of increased activity are seen scattered throughout the lung parenchyma on both sides, more on the right side. Increased activity is also identified in the right hilar region, which is thought to be a lymph node metastasis. CT scan of Chest: Innumerable bilateral calcified and noncalcified pulmonary nodules. The appearance of these pulmonary nodules is most consistent with metastatic osteosarcoma versus chondrosarcoma. |
| DDx: 1. Ossifying metastases from the distal ulnar mass. 2.Calcified metastases from unknown primary. 3. Calcified nodules from old granulomatous disease.
|
| Diagnosis: Ossifying metastases from the left distal ulnar mass. |
| References: 1.Rajendra Kumar, Ruppert David, John E. Madewell, and Marvin M. Lindell, Jr.,Radiographic spectrum of osteosarcoma; AJR 148:767-772, April 1987. 2. J-T LIN, MD, C-C YEN, MD, W-S WANG, MD, T-J CHIOU, MD and J-H LIU, MD and H-T WU, MD and P-M CHEN, MD; Case report: Unusual peritoneal spreading by metastatic osteosarcoma of the tibia; The British Journal of Radiology, 76 (2003), 337–338. 3. Veenu Singla, Vivek Virmani, Rakesh Kapoor, Ritesh Agarwal and Niranjan Khandelwal, Massive Ossified Lung Masses; Indian J Chest Dis Allied Sci 2009;51:233-235. 4. Tjeerd Zwaga, MD , Judith V. M. G. Bove´e, MD, PhD , Herman M. Kroon, MD, PhD;Best Cases from the AFIP: Osteosarcoma of the Femur with Skip Lymph Node, and Lung Metastases; RadioGraphics 2008; 28:277–283 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 324525 The reader is fully responsible for confirming the accuracy of this content. |