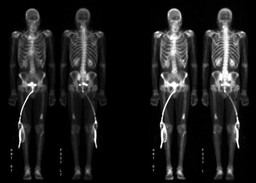
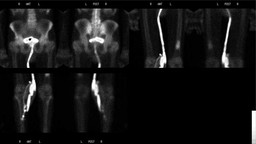
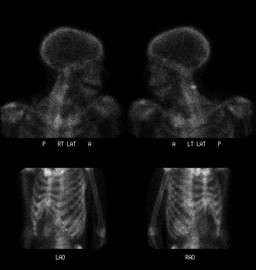
Bone metastases are often multiple at the time of diagnosis. In adults, the lesions generally occur in the axial skeleton and other sites with residual red marrow, although the lesions may be found anywhere in the skeletal system. Common sites for metastases are the vertebrae, pelvis, proximal parts of the femur, ribs, proximal part of the humerus, and skull. More than 90% of metastases are found in this distribution.
Bone scans are helpful in detecting these lesions, especially when they occur in sites that are difficult to evaluate on radiographs.
At initial presentation with prostate cancer, the value of a bone scan is limited in patients with a Gleason score of less than 7 and a prostate-specific antigen (PSA) level of less than 20 ng/mL. Those with a Gleason grade of greater than 6 may be candidates for a bone scan, irrespective of their PSA level. A bone scan may be performed as a baseline for treatment response in patients with recurrent metastatic disease at high risk of having bony metastatic disease.
Regardless of these guidelines, a bone scan is indicated in patients with prostate cancer who have symptoms suggesting bony metastases. Activity in the bone scan may not be observed until 5 years after micrometastasis has occurred; therefore, negative bone scan results do not rule out metastasis.
In addition to metastatic disease, benign bone lesions show a wide range of activity. Osteoblastomas, osteoid osteomas, chondroblastomas and giant cell tumors usually show intense activity.Enchondromas and Chondroblastomas show a moderate amount of increased activity. Fibrous cortical defects and nonossifying fibromas are usually mild or isointense compared to normal bone. Bone cysts are cold centrally but may have a warm rim due to increased bone remodelling.