|
| Patient: 77 year old male |
| History: 77 year old man admitted with worsening shortness of breath. His past medical history includes: severe COPD, paroxysmal atrial fibrillation, and ulcerative colitis. |
Image Size:
|
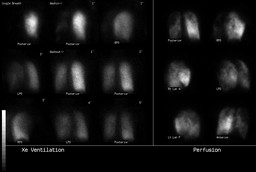
| Findings: The ventilation-perfusion scintigraphy and PA and Lateral chest x-rays performed the same day are presented Ventilation-Perfusion Scan (Fig. 1) Radiopharmaceuticals: 17.2 mCi Xe-133 gas by inhalation and 4.7 mCi Tc-99m MAA i.v.
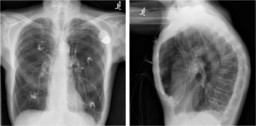
PA and lateral views of the chest (Fig. 2) The heart is normal in size. Single lead left transvenous pacer lead extends to the right ventricle. |
| DDx:
|
| Diagnosis: No Pulmonary Embolism The patient also underwent Doppler ultrasound of the lower extremities with no evidence of DVT |
| References: Diagnostic Imaging Nuclear Medicine, Morton and Clark, First Edition, AMIRSYS Carrier M et al. VIDAS D-dimer in Combination with Clinical Pre-test Probability to Rule Out Pulmonary Embolism, A Systematic Review of Management Outcome Studies. Thromb Haemost 2009;101:886-892 Agnelli and Becattini. Acute Pulmonary Embolism. NEJM 2010;363:266-74 Ceriani E et al. Clinical Prediction Rules for Pulmonary Embolism: A Systematic Review and Meta-Analysis. J Thromb Haemost 2010;8:975-70 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 293895 The reader is fully responsible for confirming the accuracy of this content. |