|
| Patient: 60 year old male |
| History: 60 year-old man with extensive local recurrence of rectal cancer after low anterior resection and chemoradiation. He underwent a revision abdominal perineal resection and radical cystoprostatectomy with ileal conduit diversion. The surgery was complicated by delayed abdominal and perineal wound healing which progressed to drainage from the perineal wound. Analysis of fluid drained from the perineum revealed a high creatinine level suggesting urine leak.
|
Image Size:
|
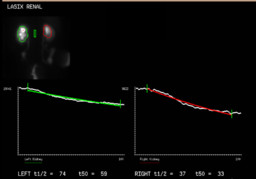
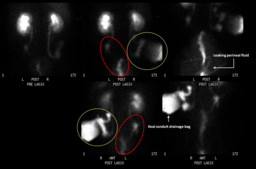
| Findings: Presented are the posterior flow and renal function images (Fig. 1) followed by posterior delayed images and anterior images after furosemide administration (Fig. 2).
Radiopharmaceutical: 8.3 mCi Tc-99m MAG3 I.V. and 40 mg furosemide I.V.
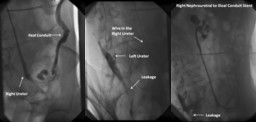
The dynamic urine flow to the ileal conduit on the right and to the perineal area on the left after furosemide administration can be appreciated on the attached cine (Fig. 6 - AVI File). The left ureter does not appear to connect with the ileal conduit and radiopharmaceutical tracks into the pelvis, most likely representing a urine leak (Fig. 4, red ellipses, best visualized on the anterior view). During this study, perineal fluid leaked onto the imaging table. This perineal fluid was found to be radioactive, further confirming the presence of a urine leak. Radiopharmaceutical is seen draining from the right ureter into the ileal conduit (Fig. 4, green circles). Diverting bilateral nephrostomies tubes were placed the day after.
|
| Diagnosis: Urine leak that is most likely secondary to disrupted anastomotic site of the left ureter to the ileal conduit diagnosed on renal scan and confirmed on antegrade ureterography. |
| References: Kawashima A, Sandler CM, Corl FM, West OC, Tamm EP, Fishman EK, Goldman SM. Imaging of renal trauma: a comprehensive review. RadioGraphics 2001; 21:557–574 Titton RL, Gervais DA, Hahn PF, Harisinghani MG, Arellano RS, Mueller PR. Urine leaks and urinomas: diagnosis and imaging-guided intervention. RadioGraphics 2003; 23: 1133-1147 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 283225 The reader is fully responsible for confirming the accuracy of this content. |