|
| Patient: 34 year old female |
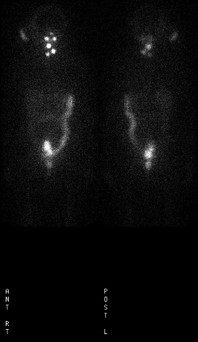
| History: 34 year old woman with T2 N0Āfollicular papillary carcinoma, status post total thyroidectomy and neck dissection. The patient received 100 mCi of I131radioactive ablationĀ5 days prior to the day of whole body I131 scintigraphy. |
Image Size:
|
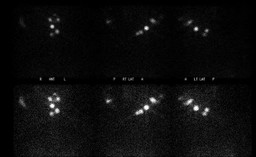
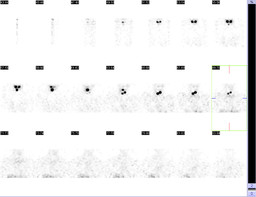
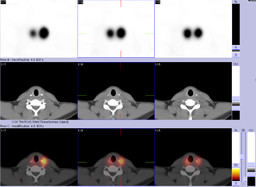
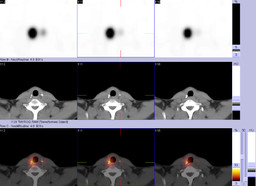
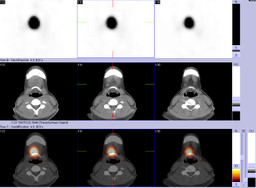
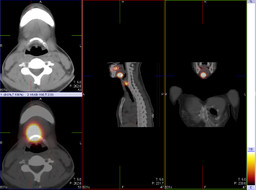
| Findings: Whole body planar I-131 scintigraphy: There is expected I-131 activity in the salivary glands, mouth and oropharynx. There are 3 foci of increasedĀradiotracer uptake. One in the midlineĀsuperior to the thyroid surgical bed, and the remaining other 2 foci more inferiorly, one being in midline and other to the left . SPECT/CT imaging for better delineation of the multiple focal areas of increased radiotracer uptake was recommended. I-131 imaging of the neck with SPECT/CT: Again seen is expected I-131 activity in bilateral submandibular glands and oral cavity. There is focal area of increased uptake anterior to the hyoid bone in theĀmidline. This area likely represents functioning thyroid tissue in the thyroglossal duct remnant. A focal area of increased uptake is identified in the region of the thyroid surgical bed, on the left side, just superior to the surgical clips. Another focal area of increased uptake is identified in the region of the surgical clips on the right side. |
| DDx: 1. Functioning thyroid tissue in the surgical bed and in a thyrogloassal duct remnant. 2. Functioning thyroid tissue in the surgical bed with regional metastatic lymph nodes. |
| Diagnosis: Probable functioning thyroid tissue inĀa thyroglossal ductĀremnant and inĀbilateral surgical bed. |
| References: 1.Ā Peretz A, Leiberman E, Kapelushnik J, Hershkovitz E. Thyroglossal duct carcinoma in children: Case presentation and review of the literature. Thyroid. 2004;14:777¢785. doi: 10.1089/1050725041872945. 2.Ā Yang YJ, Wanamaker JR, Powers CN. Diagnosis of papillary carcinoma in a thyroglossal duct cyst by fine needle aspiration biopsy. Arch Pathol Lab Med. 2000. 3.Ā Dedivitis RA, Guimareas AV. Papillary thyroid carcinoma in thyroglossal duct cyst. Int Surg. 2000;85:109¢201. 4.Ā Ruf J, Lehmkuhl L, Bertram H, et al. Impact of SPECT and integrated low-dose CT after radioiodine therapy on the management of patients with thyroid carcinoma. Nucl Med Commun 2004;25 : 1177-1182 5.Ā Tharp K, Israel O, Hausmann J, et al. Impact of I-131 SPECT/CT images obtained with an integrated system in the follow-up of patients with thyroid carcinoma. Eur J Nucl Med Mol Imaging2004; 31:1435 -1442 6.Ā Schmidt D, Szikszai A, Linke R, Bautz W, Kuwert T. Impact of 131I SPECT/spiral CT on nodal staging of differentiated thyroid carcinoma at the first radioablation. J Nucl Med. 2009;50:18¢23. 7.Ā Wong KK, Zarzhevsky N, Cahill JM, Frey KA, Avram AM. Incremental value of diagnostic 131I SPECT/CT fusion imaging in the evaluation of differentiated thyroid carcinoma. AJR Am J Roentgenol. 2008 Dec;191(6):1785-94. 8.Ā Grewal RK, Tuttle RM, Fox J, Borkar S, Chou JF, Gonen M, Strauss HW, Larson SM, Sch÷der H. The effect of posttherapy 131I SPECT/CT on risk classification and management of patients with differentiated thyroid cancer. 9.Ā Yamamoto Y, Nishiyama Y, Monden T, Matsumura M, Satoh K, Ohkawa M. Clinical usefulness of fusion of I-131 SPECT and CT images in patients with differentiated thyroid carcinoma. J Nucl Med2003; 44:1905 -1910 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 281101 The reader is fully responsible for confirming the accuracy of this content. |