|
| Patient: 67 year old male |
| History: 67-year-old man with prostate cancer. Evaluate for osseous metastatic disease. |
Image Size:
|
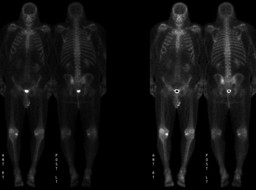
| Findings: BONE SCINTIGRAPHY (WHOLE-BODY) RADIOPHARMACEUTICAL: 20.1 mCi Tc-99m MDP i.v. Delayed whole-body scintigrams were obtained.
The images demonstrate focally increased activity in the left posterior ilium, appearing as a ring of increased activity with a central area of relatively decreased activity.
The scintigrams also demonstrate foci of mildly increased activity along the margins of the lower thoracic spine, most likely due to degenerative changes. Increased activity is also seen in the medial compartments of both knees, right greater than left, and in the patellofemoral joints, right greater than left. Small foci of increased activity are seen in the region of the left medial malleolus and the left midfoot. All of the above changes are most likely related to degenerative joint disease. The more intense uptake in the region of the right knee likely reflects the recent right knee arthroscopic surgery. There is no definite evidence to suggest osseous metastatic disease.
COMPUTED TOMOGRAPHY Rounded lucent lesion with a well-defined sclerotic margin in the left posterior ilium; the contents of this lesion were of soft tissue density.
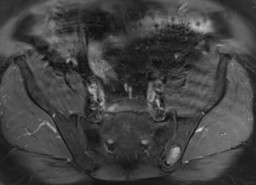
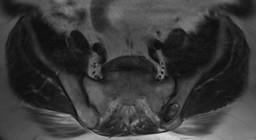
MAGNETIC RESONANCE IMAGING Rounded lesion within the left posterior ilium. The lesion is heterogenously hypo- to isointense on T2-weighted imaging and is likely enhancing on post-contrast T1-weighted imaging. Note that there are no pre-contrast T1 weighted images through this lesion, as the pelvic MRI was performed utilizing a prostate imaging protocol. Overall findings are consistent with a soft tissue lesion rather than a cystic one. |
| Diagnosis: Fibrous dysplasia of the left ilium is the most likely explanation for this finding.
This lesion was stable in appearance by comparison with bone scintigraphy and pelvic CT performed two years ealier when the prostate cancer was first diagnosed. However, the uptake on bone scintigraphy was incorrectly thought to be related to sacroiliac joint degenerative changes and the lesion on CT was thought to be a degenerative cyst. |
| References: Mettler, Fred and Milton Guiberteau. Essentials of Nuclear Medicine Imaging. 5th ed. Philadelphia, PA: Saunders Elsevier, 2006, pp 244. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 270977 The reader is fully responsible for confirming the accuracy of this content. |