|
| Patient: 28 year old female |
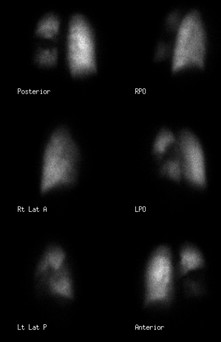
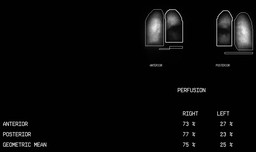
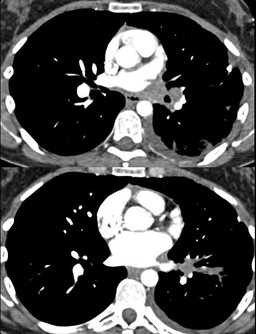
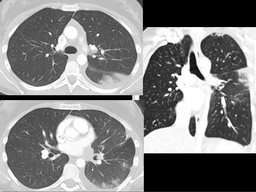
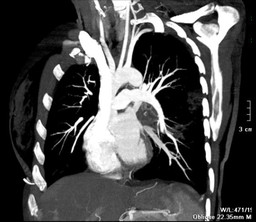
| History: 28 year-old woman with progressively worsening cough and intermittent hemoptysis over the last several months. Ā Ā Figure 1 Figure 2 Figure 3 Ā Ā What is your interpretation of this study? Ā Is this a good pattern for pulmonary embolism? Ā Ā CT Angiography: Ā Figure 4 Figure 5 Figure 6 Ā Ā Findings and interpretation?Ā |
Image Size:
|
| Findings: Chest Radiographs: Ā Bilateral lower lobe linear atelectasis. Ā Blunting of the left costophrenic angle, which may represent a small layering effusion. Ā Staple line from a prior biopsy in the left lung. Ā Left lung midlung hazy opacity is noted and may represent changes of prior biopsy Ā Ā Quantatative Lung Perfusion Scintigraphy: Ā RADIOPHARMACEUTICAL: 4.5 mCi Tc-99m MAA i.v. Ā Diffusely decreased perfusion to the left lung with absence of the superior segment of the left lower lobe. Ā The right lung receives 75% and the left lung receives 25% of total pulmonary perfusion. Ā Ā CT Chest Angiogram: Ā Bulky non-calcific soft tissue in the left hilar region and around the left pulmonary veins. The main, left, and right pulmonary arteries are normal. The left lateral basal segmental artery has a moderate stenosis approximately 3 cm away from the origin with post stenotic dilatation. The rest of the pulmonary segmental arteries are unremarkable. Ā Approximately 1 cm from the origin of left inferior pulmonary vein, there is a 40% stenosis caused by the adjacent lymphadenopathy. Approximately 2.0 cm from the origin of the left superior pulmonary vein, there is a moderate stenosis, most notable in the sagittal and axial planes, and not well seen in the coronal plane. Prominent bronchial vessels identified around the left mains stem bronchus. Ā An irregular, infiltrating left mediastinal opacity emanates into the left hilar region causing stenosis of the left inferior and superior pulmonary veins and lateral basal segmental artery, the lesion compresses the left lower lobe bronchus, superior segmental bronchus, and lateral basal segmental bronchus. Ā Postobstructive, patchy pulmonary opacities are identified in the periphery, most notable in the mid and lower lung zones. A small left pleural effusion is present. The right lung is normal. |
| DDx: DDX (Decreased Perfusion to one lung)Ā Mettler page 171 table 7-2 Ā Centrally obstructing tumor Ā Mediastinal fibrosis Ā Pulmonary agenesis or stemosis Ā Sweyer-James syndrome Ā Massive effusion Ā Aortic dissection Ā Pneumothorax Ā Pulmonary Embolism much less likely |
| Diagnosis: High grade neuroendocrine carcinoma in the left lower lobe with peribronchial, left hilar, and mediastinal lymph node metastasis (Surigical Pathology) |
| References: Aslan et al. "KI-67 IN NEUROENDOCRINE TUMORS WITH CRUSH ARTIFACT" Am J Clin Pathol 123:874-878. 2005 |
| Comments: No comments posted. |
| Additional Details:
Case Number: 245532 The reader is fully responsible for confirming the accuracy of this content. |