|
| Patient: 21 year old female |
| History: 21 year-old woman with severe post-partum cardiomyopathy Ā What device has been placed? Ā Figure 1 Figure 2 Ā TheĀdevice was placed approximately 1 year and 9 months ago and there is now purulent discharge at the drive-line skin entrance site.Ā What study would you like to perform next? Ā Figure 3 Figure 4 Ā Findings and their significance? Ā NextĀstep in management?Ā |
Image Size:
|
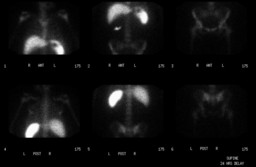
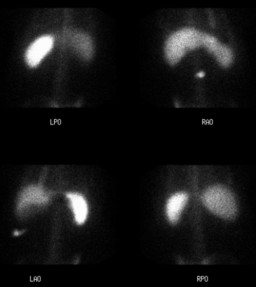
| Findings: Limited Leukocyte Scintigraphy Ā RADIOPHARMACEUTICAL: 0.46 mCi In-111 labeled autologous leukocytes i.v. Ā Focus of increased tracer uptake in the superficial anterior right mid abdomenĀ Ā Microbiology (drive Line) Ā Rare gram positive cocci Ā Follow Up Ā The patient was subsequently treated with an LVAD drive line exit site revision |
| DDx: Leukocyte scintigraphy evaluates the extent of drive-line and device involvement. Ā Exit site only Ā Exit site and drive-line Ā Exit site, drive-line, and device |
| Diagnosis: Left Ventricular Assist Device (LVAD) drive line infection, relatively superficialĀin locationĀat the skin entrance site. Ā |
| References: Pasque et al. "Surgical Management of Novacor Drive-Line Exit Site Infections" Ann Thorac Surg. 2002; 74:1267-1268. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 245518 The reader is fully responsible for confirming the accuracy of this content. |