|
| Patient: 53 year old female |
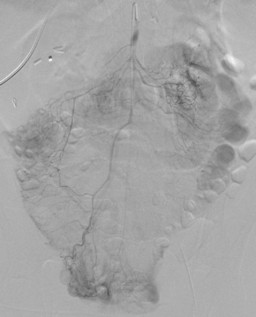
| History: 53 year old female with ischemic cardiomyopathy necesitating placement of a 2nd-generation left ventricular assist device (LVAD). The patient presents with a melena while on warfarin and clopidogrel. See figures 1-3
What is your interpretation of this study and what is the next step in management?
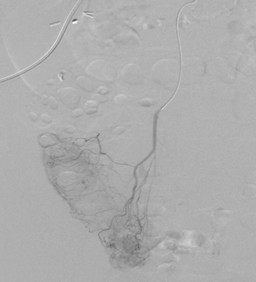
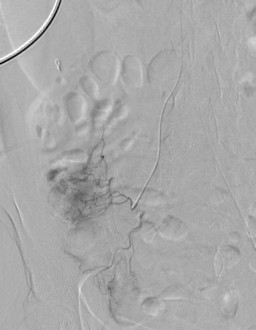
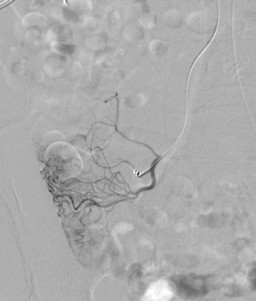
Findings and intervention performed? (figures 4-9)
What additional procedure may be helpful in determining a diagnosis? (see figure 10)
|
Image Size:
|
| Findings: Gastro-intestinal Bleeding Scintigraphy: RADIOPHARMACEUTICAL: 26.8 mCi Tc-99m in vitro labeled red cells i.v. Lower gastrointestinal hemorrhage, specifically arising from the region of the cecum.
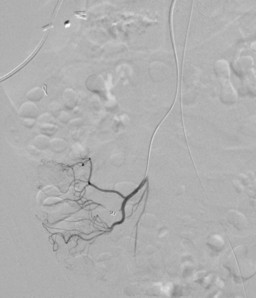
Angiography: Coil embolization of distal branch of the ileocolic artery supplying the bleeding segment of the cecum. No evidence of active bleeding on the post coiling angiograms.
Colonoscopy: See figure 10 and general discussion |
| DDx: Dieulafoy lesion
Angiodysplasia
Other causes of lower gastrointestinal bleeding:
Diverticular disease
Telangectasias
Neoplasms
Advanced liver disease causing mucosal spider nevi
|
| Diagnosis: Dieulafoy Lesion |
| References: Jain, Richa and Chetty, Runjan. "Dieulafoy Disease of the Colon." Arch Pathol Lab Med. 133; 1865-1867, 2008. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 245472 The reader is fully responsible for confirming the accuracy of this content. |