General Discussion: Full Patient History:
61-year-old man with left squamous cell tonsillar carcinoma status post radical pharyngectomy and base of tongue resection with known invasion of the left carotid artery. Radiation therapy has a risk of left carotid artery injury. Therefore, left carotid artery balloon occlusion was performed to evaluate for significant drop in cerebral perfusion
General Discussion:
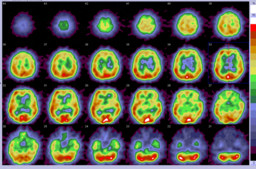
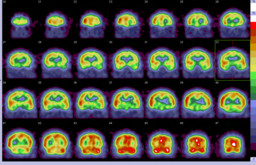
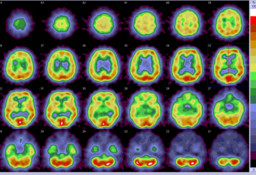
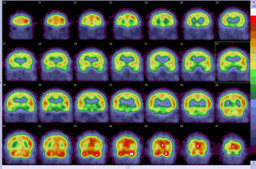
Temporary balloon-occlusion SPECT using Tc-99m bicisate or Tc-99m HMPAO allows evaluation of cerebral vascular reserve for potential carotid artery sacrifice.
Normal cerebral blood flow (CBF) is approximately 55 ml/100 g/min. Neuronal dysfunction and cerebral ischemia develop when CBF drops below about 20 ml/100 g/min with cerebral infarction occurring when CBF falls below 10 ml/100 g/min. The appearance of a neurologic deficit during balloon occlusion of the ICA, with simultaneous neurologic examination, indicates that CBF has fallen below the critical threshold necessary to maintain neuronal function and is considered unequivocal evidence that the patient will not tolerate ICA occlusion. Unfortunately the failure to develop neurologic defects during temporary balloon occlusion does not ensure the safety of the procedure and stroke rates of up to 20% following a negative temporary balloon occlusion have been reported. Thus Tc-99m bicisate or Tc-99m HMPAO SPECT is useful in assessing significant drop in perfusion in asymptomatic patients.
In this case, the patient did not demonstrate any decline in his neurological status during 30 minutes of occlusion. The occlusion study (SPECT Day #1) demonstrated 10-20% drop in cerebral perfusion in the left hemisphere, compared to the right. The baseline study (SPECT Day #2) performed the next day showed symmetrical perfusion. This suggests that the perfusion asymmetry seen on the occlusion study was due to carotid artery occlusion. However, because of limited treatment alternatives, the patient subsequently received complete embolization of the cervical segment of left internal carotid artery. Before discharge, he developed transient right sided facial drop and weakness with low blood pressure, indicating low cerebral vascular reserve in the left hemisphere. The patient was discharged on anticoagulation therapy.