General Discussion: Full Patient History:
The patient is a 57-year-old woman with hypercalcemia and hyperparathyroidism. The patient had a prior right parathyroidectomy for hyperparathyroidism, as well as right thyroidectomy. The patient is on Synthroid for hypothyroidism.
General Discussion:
Hyperparathyroidism occurs with a frequency of 5 per 10,000. About 80% to 85% of cases of primary hyperparathyroidism are due to single or multiple hyperfunctioning adenomas. Hyperplasia accounts for about 15% of cases and parathyroid carcinomas for about 1-3%
About 80% to 85% of parathyroid adenomas are found adjacent to the thyroid. Ectopic parathyroid adenomas can be found in the anterior or posterior superior mediastinum, within or next to the thymus, along the esophagus, along the carotid sheath, or at the carotid bifurcation. Parathyroid scintigraphy with Tc-99m Sestamibi is commonly part of pre-operative work-up, to help localize adenoma for surgical resection.
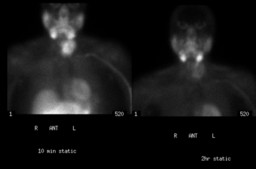
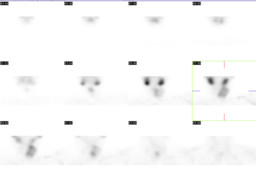
Sestamibi (Cardiolite) is an lipophilic cationic isonitrile that passively enters into cellular cytosol and actively concentrate in mitochondria. On parathyroid scintigraphy, Tc-99m Sestamibi initially concentreates in normal thyroid tissue, thyroid adneomas, parathyroid adenomas, and hyperplastic parathyroid glands. Over time (2 hours), there is significant wash-out in the normal thyroid tissue. Thyroid adenomas and hyperplastic parathyroid glands initially have more intense activity than does the thyroid, but they also typically fade with time. Parathyroid adenomas, on the other hand, tend to have more intense initial activity, and retain the radiotracer for longer period of time. Repeat imaging at 2 hours after radiotracer injection can often demonstrate any present parathyroid adenoma, with sensitivity of about 90% in primary hyperparathyroidism. Thyroid cancerĀand parathyroid carcinoma can also have increased and persistent sestamibi uptake, and should be considered in the differential diagnoses.
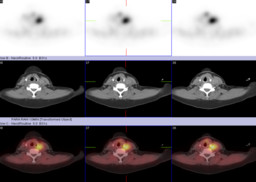
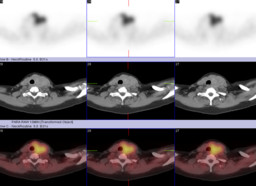
In this case, there is initial patchy sestamibi uptake in the left thyroid gland, corresponding to multiple nodules seen on CT (Figure 4), as well as ultrasound (not shown). In addition, there is a small focus of persistent activity in the superior left thyroid bed, corresponding to a nodule on CT (Figure 1, Figure 3). This nodule was proven to be parathyroid adenoma on surgical pathology. Left thyroidectomy showed no cancer. Patient's serum calcium and parathyroid hormone normalized after surgery.
Ā