General Discussion: Full Patient History
The patient is an 18-year-old girl who presented with a 3-month history of right lower extremity pain without prior injury or surgery. She has been experiencing episodes of pain in her right anterior distal thigh just above her knee. The pain was initially dull and mild, not requiring medications or medical attention. Then she experienced worsening of her complaints. The pain has spread to involve her entire right thigh, knee, and leg. There is also similar pain in her left thigh. The pain is associated with episodic color changes where her thigh turns purple for minutes to several hours and then returns back to normal color. She also noticed that her right lower extremity is generally cooler to the touch compared to the left. She reports numbness and tingling sensation in her right foot as well as in the lateral aspect of her right leg and thigh.
General Discussion
Complex Regional Pain Syndrome (CRPS) is a chronic progressive disease characterized by severe pain, swelling, changes in the skin, and vasomotor instability in the affected limb. The International Association for the Study of Pain has divided CRPS into two types based on the presence of nerve lesion following the injury.
- Type I, formerly known as reflex sympathetic dystrophy (RSD), Sudeck's atrophy, reflex neurovascular dystrophy (RND) or algoneurodystrophy, does not have demonstrable nerve lesions
Type II, formerly known as causalgia, has evidence of obvious nerve damage.
The pathophysiology of CRPS is not fully understood. "Physiological wind-up" and central nervous system (CNS) sensitization, are key neurologic processes that appear to be involved in the induction and maintenance of CRPS. There is compelling evidence that the N-methyl-D-aspartate (NMDA) receptor has significant involvement in the CNS sensitization process. It is also hypothesized that elevated CNS glutamate levels promote "physiological wind-up" and CNS sensitization
Precipitating factors include injury and surgery, although there are documented cases that have no demonstrable injury to the original site.
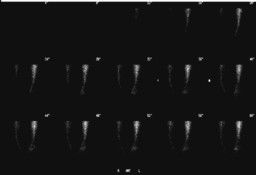
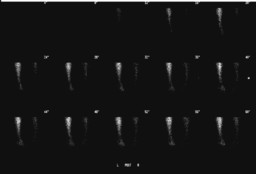
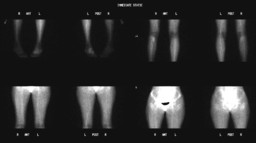
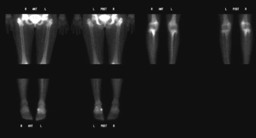
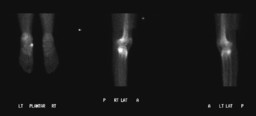
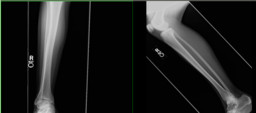
On radiograph, there is usually patchy periarticular osteoporosis. On bone scan, three-phase bone scan classically demonstrates increased blood flow to the affected limb with increased asymmetric periarticular radionuclide activity. Delayed images typically show increased radiopharmaceutical uptake around all joints in the affected limb. However, about 1/3 of adult patients with clinical presentation of CRPS do not show increased perfusion and uptake. Children with CRPS commonly have decreased blood flow with decreased radiopharmaceutical uptake in the affected limb, thought to be related to vasoconstriction, as in this case.