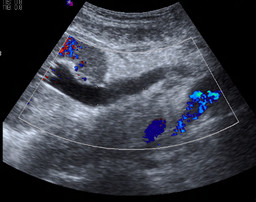
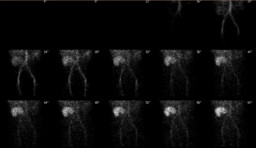
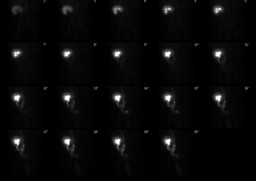
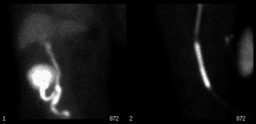
| Findings: RENAL SONOGRAM: Moderate hydronephrosis and hydroureter within the right transplant kidney. Ā RENAL SCINTIGRAPHY: RADIOPHARMACEUTICAL: 7.5 mCi Tc-99m MAG 3 and 40 mg furosemide i.v. FINDINGS: The anterior pelvic radionuclide angiogram demonstrates normal perfusion of the transplanted kidney in the right iliac fossa. The initial images demonstrate normal transplant size, morphology, and tracer accumulation. The sequential imagesĀshow prompt uptake and excretion of the radiopharmaceutical by the transplant. The pelvicalyceal system of the transplantĀappears mildly dilated. Note also is made of reflux into the native right ureter via the uretoureteric anastomosis. The transplant ureter and the native ureter appear prominent. No abnormalities of the bladder are seen, and there is excretion of the tracer into the Foley catheter drainage bag. There is no evidence for urine extravasation or perirenal mass. To evaluate for obstruction, the patient was given 40 mg furosemide via slow intravenous injection approximately 30 minutes after the start of the examination. Sequential images were obtained for an additional 20 minutes. There is prompt clearance of pelvicalyceal activity from the kidney after diuretic administration.ĀA single static posterior image taken at the end of the examination additionally demonstrated activity within the native right renal collecting system, as a result of reflux. |