| Additional Details:
Case Number: 173604 Owner(s): Joanna Fair and Jerold Wallis, Assoc Prof of RadiologyLast Updated: 02-07-2013 Owner(s): Joanna Fair and Jerold Wallis, Assoc Prof of RadiologyLast Updated: 02-07-2013
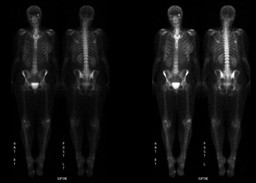
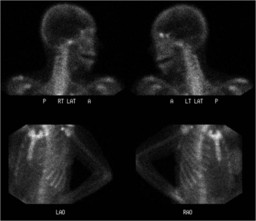
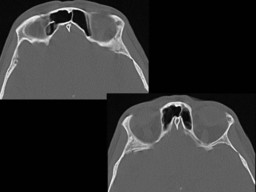
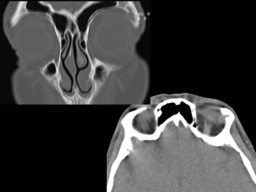
Anatomy: Skeletal System Pathology: Benign Mass, Cyst
Modality: CT, MR, Nuc MedAccess Level: Readable by all users, writable by NucMed Certifiers
Keywords: bsnm, bone scintigraphy, ossifying fibroma, fibro-osseus lesion, fibrous dysplasiaACR: 40000.31390
Case has been viewed 33 times.
Certified by Jerold Wallis on 06-24-2009The reader is fully responsible for confirming the accuracy of this content.
Text and images may be copyrighted by the case author or institution.
|