General Discussion: Metaiodobenzylguanidine (MIBG) is used to evaluate extent of disease in children with neuroblastoma and can be labeled with I-131 or I-123, the latter has more favorable dosimetry and image quality. Patient preparation includes pretreatment with iodine to prevent thyroid uptake of free radioactive iodine. MIBG is taken up in presynaptic neurons similar to norephinephrine. MIBG is normally taken up in the liver, spleen, salivary glands, thyroid, and heart. The radiotracer is excreted in the urine which resulting in bladder and kidney activity on imaging. Diffuse lung activity, bowel activity, and uptake within brown fat can also be seen. Multiple medications can interfere with MIBG uptake which is often an issue with adults but seldom in children. Imaging is typically preformed 24 hours after injection.
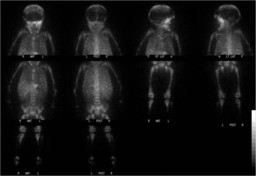
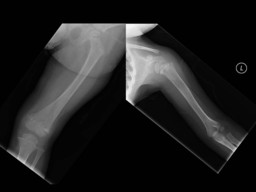
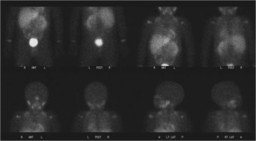
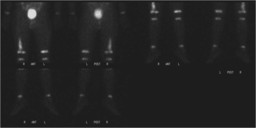
This patient presented with extensive skeletal disease that resulted in relative decreased radiotracer uptake in the liver, spleen, salivary glands and heart. X-rays of extremities show permeative bone destruction consistent with osseous metastatic disease (Figure 2). CT scan shows the primary neuroblastoma superior to the left kidney (Figures 3 and 4). The patient was subsequently treated and showed improvement on follow up imaging with some residual disease in multiple epiphysis and distal right leg (Figures 5 and 6). This patient was also treated with therapeutic doses of I-131 MIBG which is available at some centers.