|
| Patient: 30 year old female |
| History: 30 year old female: Chronic left heel pain. |
Image Size:
|
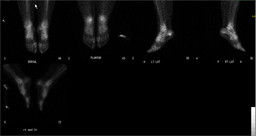
| Findings: RADIOPHARMACEUTICAL: 21.6 mCi Tc-99m MDP i.v. FINDINGS: The lateral foot radiograph is normal. On delayed bone scan images of the feet and ankles, there is a small focus of increased radiotracer uptake at the inferior aspect of left calcaneous at the expected origin of the plantar fascia. |
| DDx: Plantar fasciitis. |
| Diagnosis: Plantar fasciitis. |
| References:
Ozdemir H, Ozdemir A, Soyucu Y, Urguden M. The role of bone scintigraphy in determining the etiology of heel pain. Ann Nucl Med. 2002 Sep;16(6):395-401. Foster C, Vu D, Van der Wall H, Perera C, Halasz P, Emmett L, Fogelman I. scintigraphy predicts outcome of steroid injection for plantar fasciitis. J Nucl Med 2006; 47:1577-80. |
| Comments: No comments posted. |
| Additional Details:
Case Number: 144857 The reader is fully responsible for confirming the accuracy of this content. |