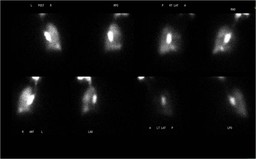
The first set of nuclear medicine images are from a ventilation study using Tc-99m labeled DTPA aerosol (Figure 2). The radiotracer is inhaled and normally deposited in respiratory bronchioles and alveoli. In patients with turbulent airflow, there can be deposition of the aerosol within the central airways as is seen in this patient within the right central bronchi.
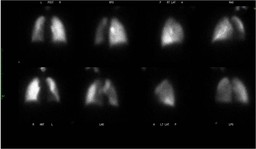
The second set of nuclear medicine images are from a perfusion study using Tc-99m labeled MAA which was injected intravenously (Figure 3). These particles normally become lodged in the pulmonary capillary bed because of their size, which results in an image displaying the regional perfusion to the lungs.
The finding of absent ventilation with preserved perfusion within the lung isknown as “reverse ventilation-perfusion mismatch” and indicates a functional right-to-left shunt. Blood is passing though the left lung without being adequately oxygenated which results in systemic hypoxia. The mildly decreased flow to the left lung on the perfusion study is likely secondary to some physiologic pulmonary arterial vasoconstriction due to the low oxygen concentration within non-ventilating left lung. However, the maintenance of perfusion to this lung indicates an inadequate hypoxic vasoconstriction reflex.
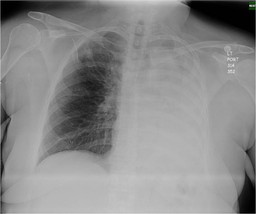
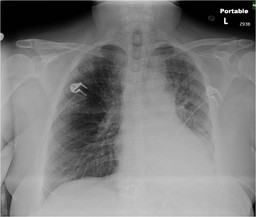
Also of note in this patient is that the scintigraphic findings do not correlate well with the findings on the chest radiograph, which shows aeration of the left upper lobe (Figure 1). This chest radiograph was taken 23 hours before the V/Q scan. A chest radiograph taken within 2 hours of the V/Q scan shows complete opacification and some volume loss of the entire left lung which correlates, well with the V/Q scan (Figure 4).
“Reverse ventilation-perfusion mismatch” is most often caused by obstruction of the airway, most commonly secondary to a mucus plug. In this case brochoscopy was performed and confirmed the presence of a large mucus plug. Follow-up chest radiography after removal of the mucus plug shows improved opacification of the left lung (Figure 5). Cultures from the brochoscopy showed that the left lower lobe opacity represented pneumonia.